Prostate Cancer Statistics and Facts: 2025 Insights




Article Summary
- Prostate cancer statistics are important to understand what to expect from the disease.
- Its incidence is higher as we age, especially in African American men living in developed countries.
- Prostate cancer death rate is not very high but can be increased by different factors such as the Gleason and TNM score, the extent of the tumor, and the age of diagnosis.
Prostate cancer is one of the most common cancers affecting men, most notably those over 60.
Ongoing research has deepened our global understanding of this disease, making it vital to stay informed about the latest statistics and insights.
We’ve collected the most essential prostate cancer statistics, including risk factors, survival rates, and critical facts you need to know about the current state of prostate cancer.
In our comprehensive analysis of prostate cancer statistics, we’ve drawn from globally respected sources like SEER, WHO, and GLOBOCAN, supported by peer-reviewed research. Reviewed by medical experts to ensure accuracy and transparency, this data-driven article presents up-to-date, ethically gathered insights while acknowledging limitations such as data lag and regional healthcare disparities.
Committed to providing the most current information, we regularly update this page as new data emerges, helping readers stay informed on key prostate cancer trends.
How Common is Prostate Cancer?
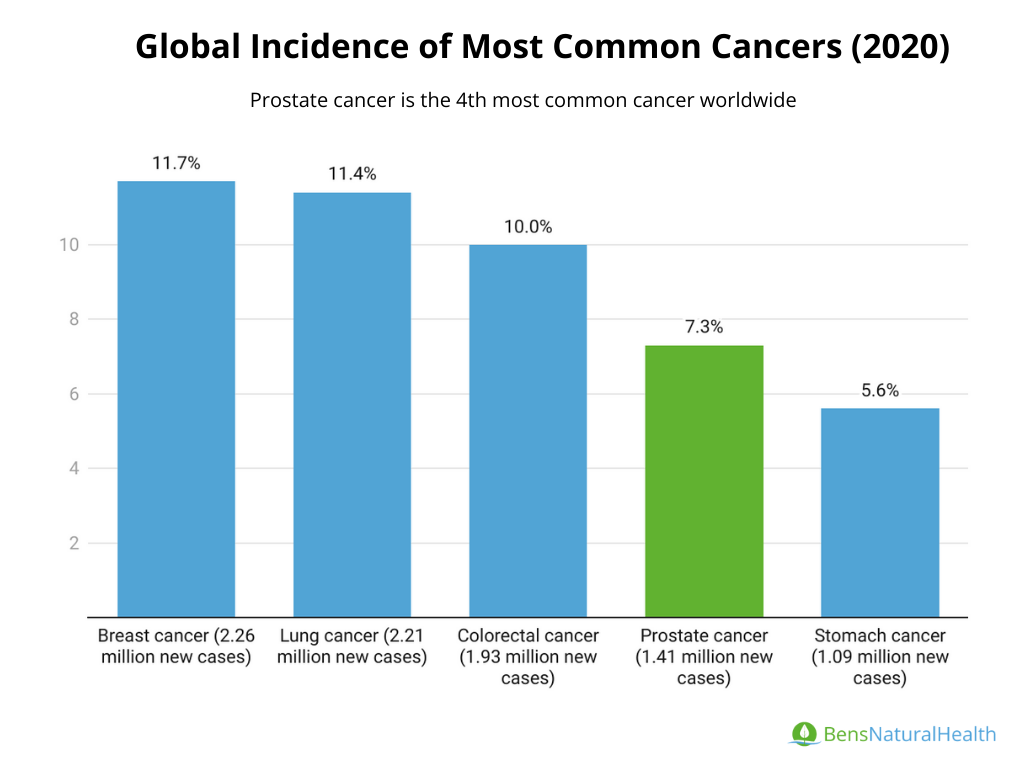
- Prostate cancer is the 4th most common cancer worldwide.
- It ranks as the second most diagnosed cancer in men after lung cancer.
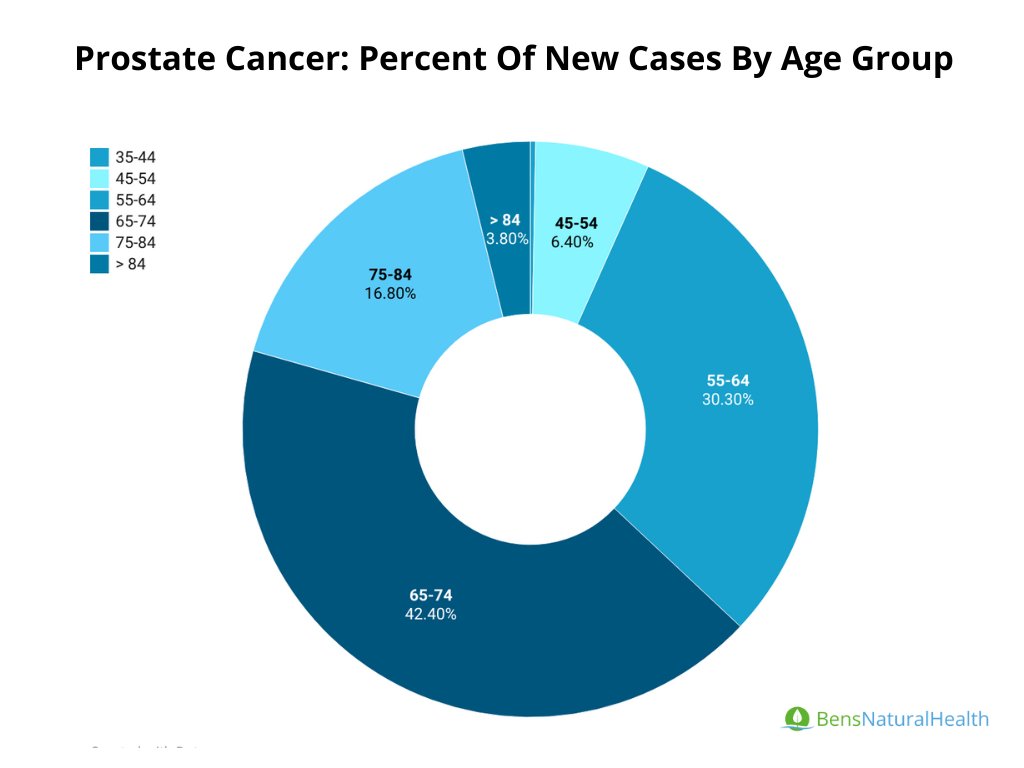
- Prostate cancer is most frequently diagnosed among men aged 65–74.
- Localized prostate cancer survival rates:
- 5-year survival rate is over 99%
- 10-year survival rate is 98%.
- 15-year survival rate is about 91%
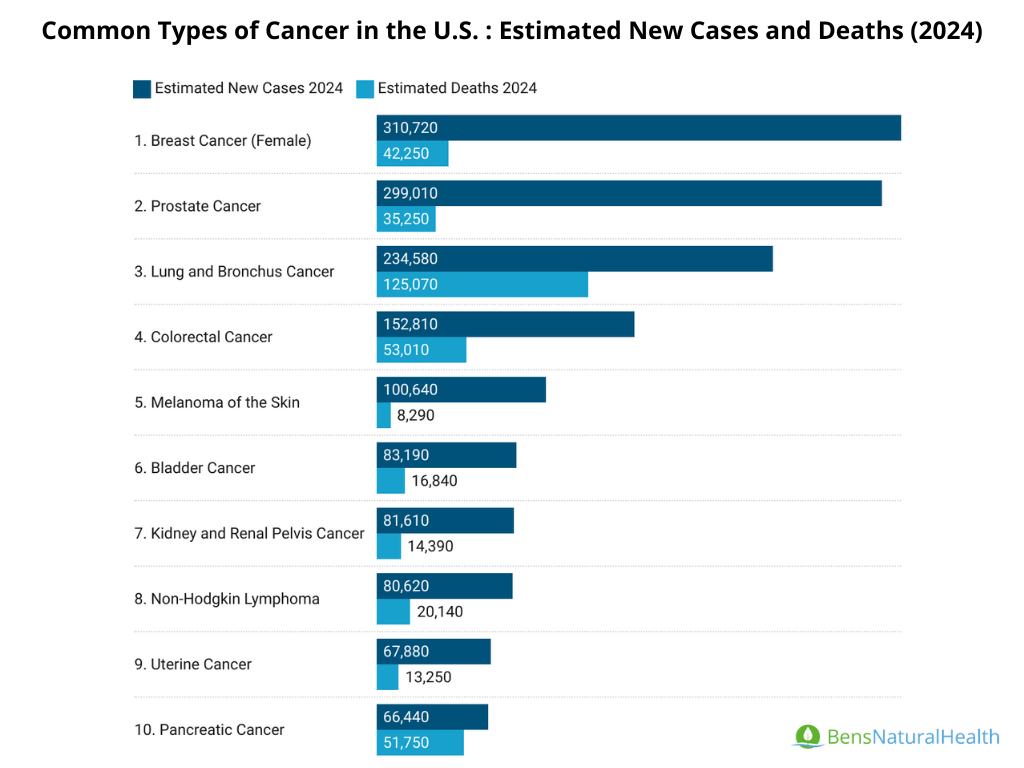
- The American Cancer Society’s estimations for prostate cancer in the United States for 2024:
- 299,010 new cases of prostate cancer
- 35,250 deaths from prostate cancer
About 1 in 8 men in the U.S. will be diagnosed with prostate cancer at some point during their lifetime.
Prostate cancer is a significant health concern globally, with different incidence and mortality rates influenced by factors such as healthcare access and screening practices.
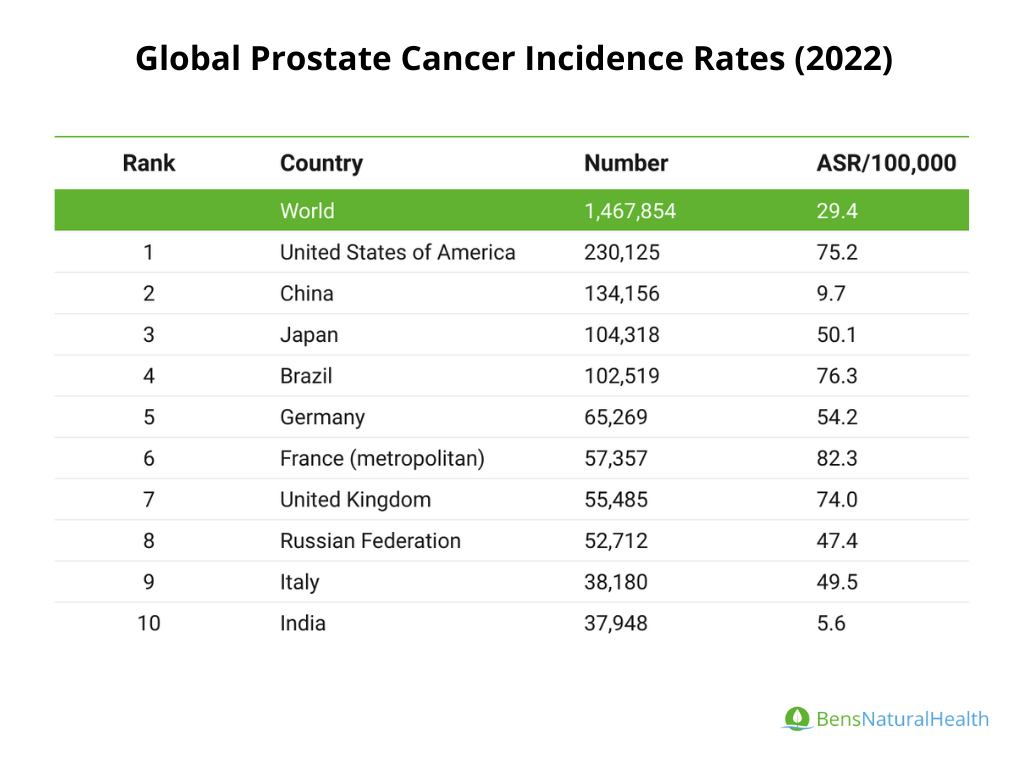
Incidence: In 2020, there were about 1.41 million new cases of prostate cancer globally. This data aligns closely with the 1,467,854 cases reported in 2022.
- The global age-standardized incidence rate is about 29.4 cases per 100,000 men, but this figure masks significant regional differences.
- In countries like the USA and France, the rates soar to 75.2 and 82.3 cases per 100,000, respectively, reflecting better screening and diagnosis.
Lifetime Risk: The lifetime risk of a man being diagnosed with prostate cancer is estimated at 1 in 8 (12.5%) in developed nations like the United States. However, this high risk is not mirrored in developing regions, where lower detection rates are often attributed to inadequate screening practices, leading to underdiagnosis.
Mortality Rates: The total global deaths from prostate cancer reached 397,430 in 2022, a slight increase from over 375,000 in 2020.
- The global mortality rate stands at 7.3 deaths per 100,000 men, but this figure is disproportionately low compared to countries like Nigeria, which reports a mortality rate of 27.9 deaths per 100,000.
This discrepancy suggests that certain regions face a much higher risk of dying from the disease, likely because of late diagnoses and limited treatment options.
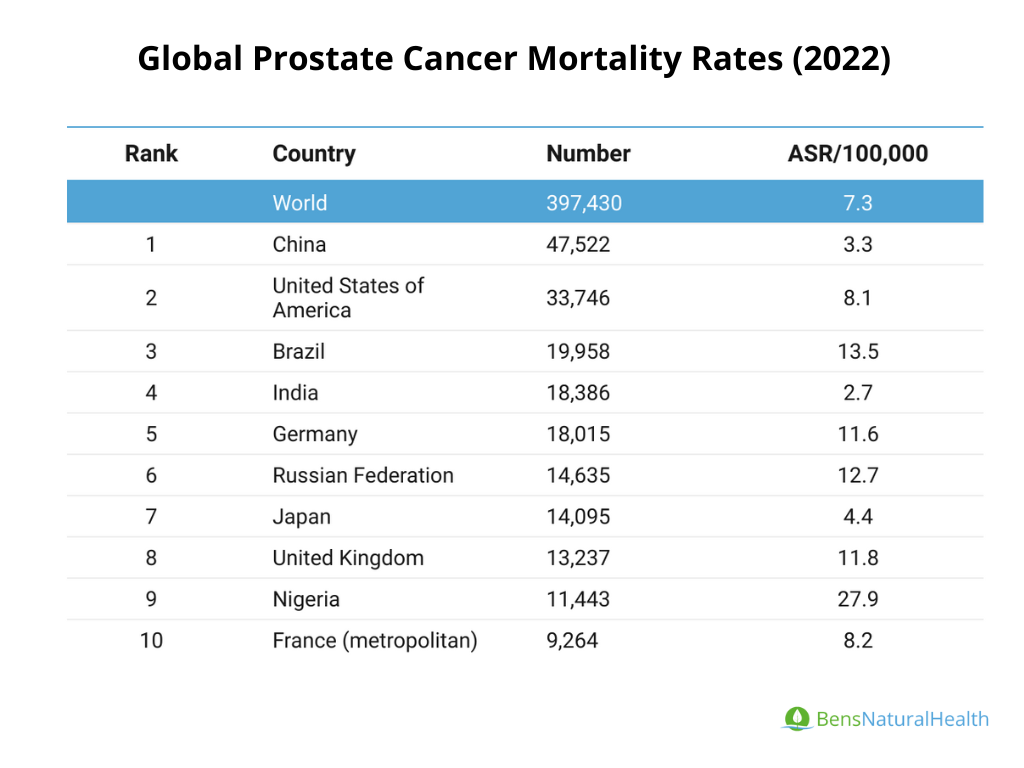
Country-Specific Data: For example, the incidence rate in China is reported at 9.7 per 100,000, while the mortality rate is lower at 3.3 per 100,000. This may indicate that prostate cancer is diagnosed less frequently, and the majority of those diagnosed survive the disease. However, additional factors, such as variations in healthcare access, diagnostic practices, or cancer biology, could also influence these statistics.
Screening Practices: The differences in diagnosis rates highlight the importance of screening. In North America and Europe, where screening is more prevalent, prostate cancer is diagnosed more frequently compared to developing countries, where limited access to healthcare can lead to underreported incidence rates. This underlines the need for improved awareness and screening in regions with lower diagnosis rates to better address and manage prostate cancer.
Percentage of Men Who Get Prostate Cancer
Globally, the percentage of men who will be diagnosed with prostate cancer is different by region due to differences in screening, genetics, and environmental factors. Here are some key prostate cancer statistics:
United States:
- Prostate cancer is the most common cancer in men in the U.S. (excluding skin cancers), according to the American Cancer Society (ACS).
- In 2024, an estimated 299,010 new cases of prostate cancer will be diagnosed in the U.S., according to the American Cancer Society (ACS).
About 1 in 8 men in the U.S. will be diagnosed with prostate cancer at some point during their lifetime.
Europe:
- In Europe, prostate cancer is also highly prevalent. It is the most commonly diagnosed cancer in men in several countries.
- Incidence rates vary across European nations, with higher rates in Northern and Western Europe. For example:
- Sweden and Norway have among the highest incidence rates, partly due to widespread PSA screening.
In 2020, there were approximately 473,000 new cases of prostate cancer in Europe.
Risk of Prostate Cancer by Age
Age is one of the most significant risk factors for prostate cancer. The likelihood of developing the disease increases as men age, with most cases being diagnosed in older men.
- Men aged 65 and older are at the highest risk, with the vast majority of cases diagnosed after this age, particularly after age 70.
- Prostate cancer is most frequently diagnosed among men aged 65–74.
Here is a more detailed breakdown of the risk:
- Under 40 years old: Prostate cancer is extremely rare in this age group.
- Ages 40–59: Risk starts to increase but remains relatively low. About 1 in 38 men are diagnosed within this age range.
- Ages 60–69: based on a data from Prostate Cancer Foundation, the risk becomes more pronounced, with approximately 1 in 19 men diagnosed in this age group.
- Ages 70 and older: The highest risk, with about 1 in 11 men diagnosed in this age group. The average age at diagnosis is 66 years old, according to the National Cancer Institute.
Prostate Cancer Risk by Ethnicity
Prostate cancer incidence and mortality rates differ significantly by race and ethnicity, with some populations being at much higher risk than others.
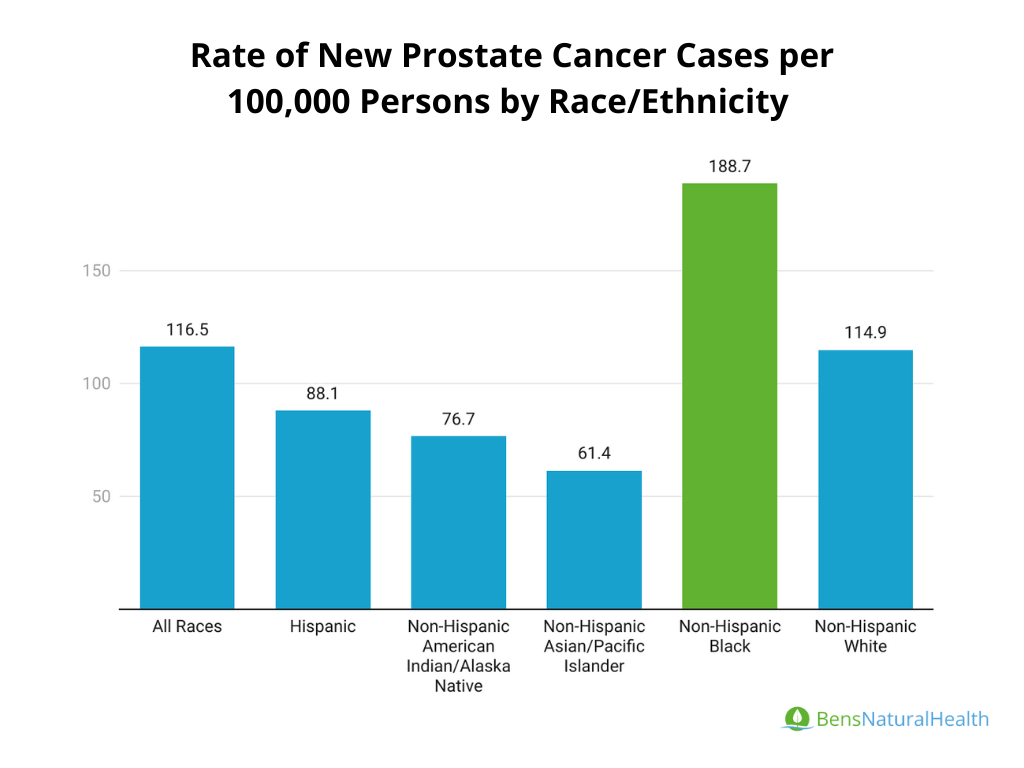
- African American men have the highest incidence of prostate cancer. They are about 1.7 times more likely to develop the disease compared to White men. Additionally, African American men are more than twice as likely to die from prostate cancer.
- White men have a lower incidence but still face significant risks, with 1 in 8 White men being diagnosed with prostate cancer at some point in their life.
- Hispanic/Latino men tend to have lower prostate cancer rates compared to non-Hispanic White men.
Asian and Pacific Islander men: Have the lowest incidence of prostate cancer among racial/ethnic groups in the U.S.
Genetic and Hereditary Factors Statistics
Family history is a significant risk factor for prostate cancer, and specific genetic mutations can increase a man’s risk.
- Hereditary prostate cancer (inherited genetically) accounts for about 5-10% of all prostate cancer cases.
- Familial prostate cancer (occurring more often in families than expected by chance) accounts for 15-20% of cases.
- If a man has a father or brother with prostate cancer, his risk of developing the disease is 2-3 times higher than that of the average man.
- Having multiple relatives with prostate cancer further increases the risk.
- Genetic mutations like BRCA1 and BRCA2, which are commonly associated with breast cancer, can also increase the risk of developing aggressive prostate cancer.
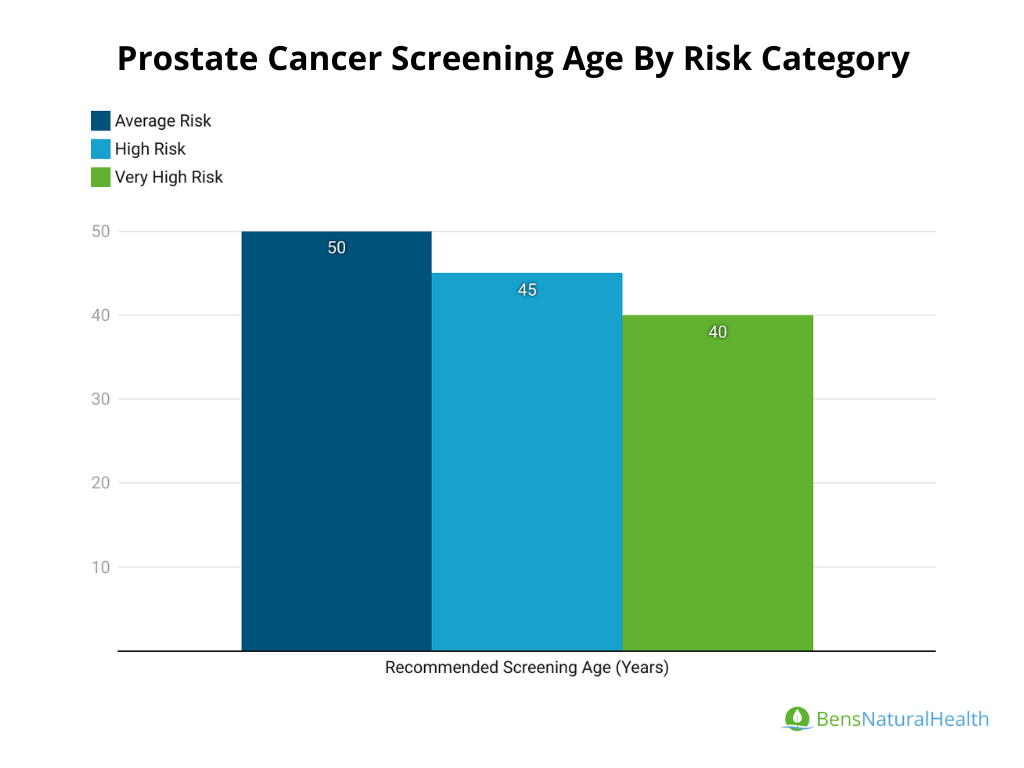
Prostate Cancer Screening Age
The age at which men should begin prostate cancer screening depends on their risk factors:
- Average Risk: The American Cancer Society (ACS) recommends that men with average risk start discussions with their doctor about screening at age 50.
- High Risk: Men who are at higher risk, including African American men and those with a family history of prostate cancer, should begin discussions about screening at age 45.
- Very High Risk: Men with multiple first-degree relatives (e.g., father, brother) diagnosed with prostate cancer at an early age (before 65) are considered to be at very high risk and should start discussing screening at age 40.
Screening is typically conducted through a prostate-specific antigen (PSA) blood test and a digital rectal exam (DRE). Early detection through screening can significantly improve outcomes for men diagnosed with prostate cancer.
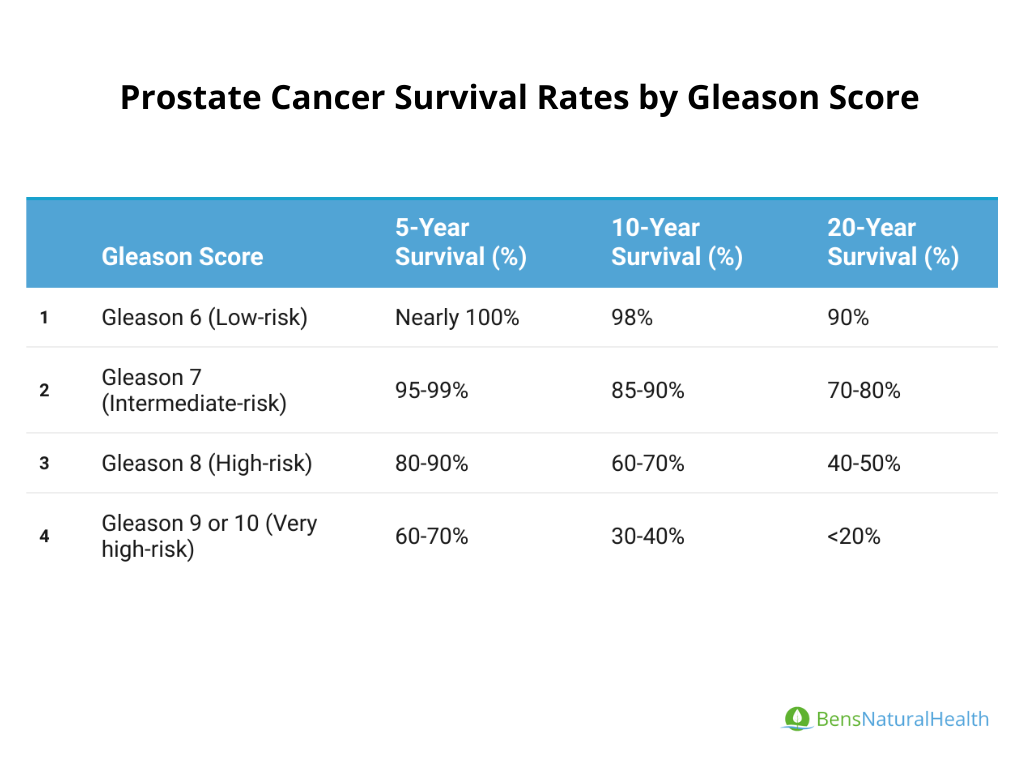
Prostate Cancer Survival Rate Statistics
Let’s start with the Gleason score statistics; survival rates by Gleason score provide insight into how aggressive the cancer is and the likelihood of successful treatment:
Prostate Cancer Survival Rate Statistics By Period
Survival rates for prostate cancer differ based on time since diagnosis. Let’s explore the prostate cancer survival statistics based on period to understand how outcomes differ over time:
5-Year Survival Rate:
- According to more recent sources, the 5-year survival rate for localized prostate cancer is over 99%, meaning there is virtually no excess mortality compared to the general population.
- In a different regional study in Iran, the overall 5-year survival rate was 82%, with significantly higher rates among patients who received combined radiotherapy and surgery.
10-Year Survival Rate:
- For patients with localized prostate cancer, the 10-year survival rate is approximately 98%.
- Another study found 10-year disease-free survival rates after combined seed implant and external irradiation to be 83%, with 93% for low-risk patients.
15-Year Survival Rate:
For men with clinically localized prostate cancer treated with observation or androgen withdrawal therapy, the 15-year survival rate is approximately 91%, with a stable mortality rate beyond this period.
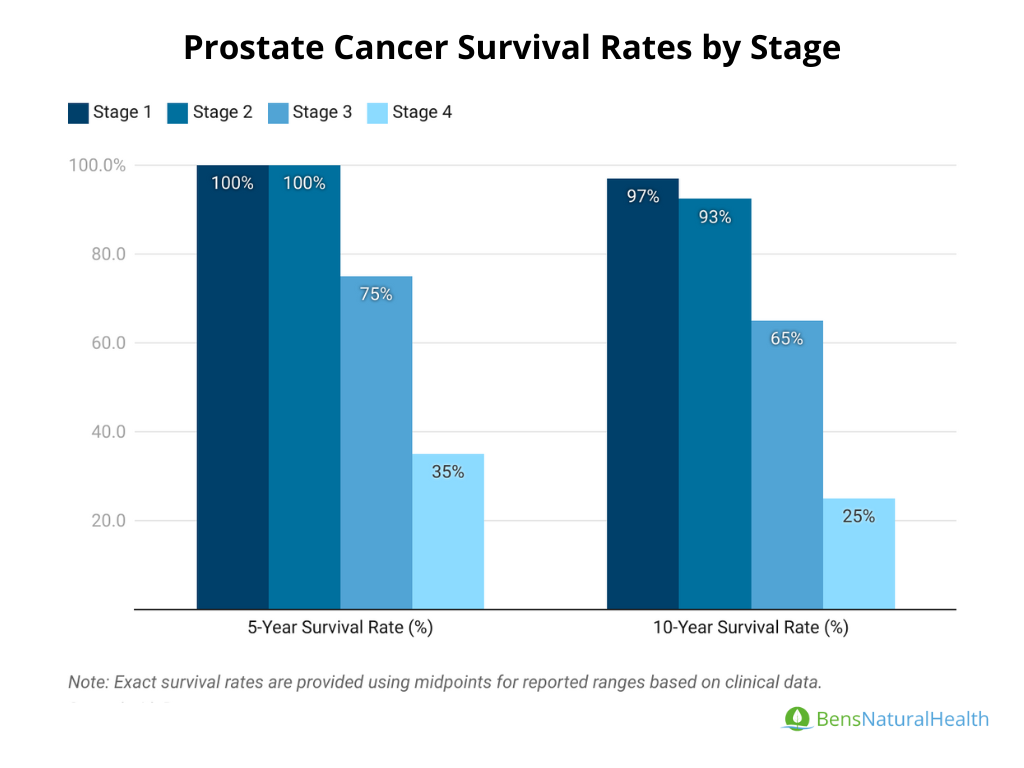
Prostate Cancer Survival Rate by Stage
Here are the key statistics on prostate cancer survival rate based on stages:
Stage 1 Prostate Cancer Survival Rate:
- 5-Year Survival Rate: Close to 100%.
- 10-Year Survival Rate: Approximately 95-98% for patients diagnosed at Stage 1.
Stage 2 Prostate Cancer Survival Rate:
- 5-Year Survival Rate: Nearly 100%, with excellent outcomes when treated early.
- 10-Year Survival Rate: Approximately 90-95%, depending on the aggressiveness of the tumor and treatment choices.
Stage 3 Prostate Cancer Survival Rate:
- 5-Year Survival Rate: Around 70-80%, as cancer has spread outside the prostate but not to distant organs.
- 10-Year Survival Rate: Estimated 60-70%.
Stage 4 Prostate Cancer Survival Rate:
- 5-Year Survival Rate: Approximately 30-40%, as the cancer has spread to distant organs.
10-Year Survival Rate: Between 20-30%.
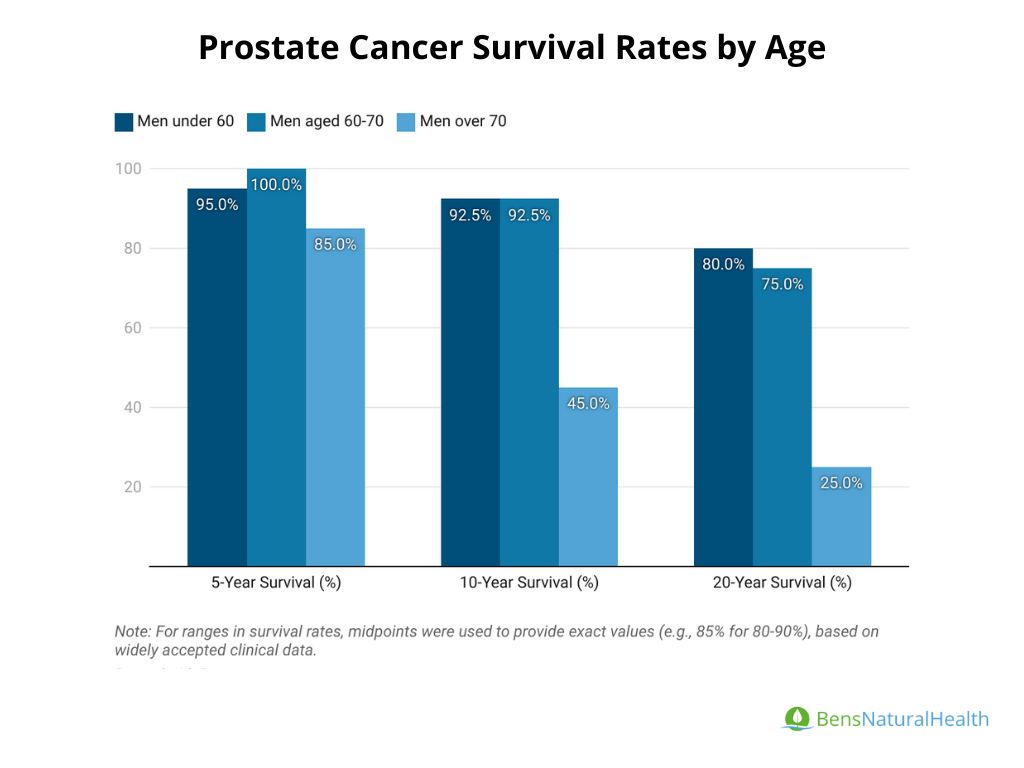
Prostate Cancer Survival Rate by Age
- Men under 60 years old:
- 5-Year Survival Rate: Approximately 97.5% for localized prostate cancer.
- 10-Year Survival Rate: 90-95% for early-stage cancers.
- 20-Year Survival Rate: Around 80%, depending on the stage and treatment approach.
- Men aged 60-70 years:
- 5-Year Survival Rate: Nearly 100% for localized prostate cancer.
- 10-Year Survival Rate: Approximately 90-95% for early-stage cancers.
- 20-Year Survival Rate: About 70-80%, decreasing as the cancer advances or with comorbid conditions.
- Men over 70 years old:
- 5-Year Survival Rate: 80-90% for localized prostate cancer.
- 10-Year Survival Rate: 40-50% due to higher incidence of aggressive tumors and comorbidities.
20-Year Survival Rate: Significantly lower, typically around 20-30% for advanced cases.
Prostate Cancer Treatment Success Rate Statistics
Prostate cancer treatments like surgery, radiation, and hormone therapy have high success rates for early-stage cancer, while advanced cases require complex management with lower cure rates.
- Surgery (Radical Prostatectomy): Nearly 100% 5-year survival for localized prostate cancer.
- Proton Therapy: 5-year biochemical disease-free survival: 88% for early-stage prostate cancer, with fewer side effects than traditional radiation. Typically requires 39-44 treatments.
- High-Intensity Focused Ultrasound (HIFU):
- 5-year failure-free survival: 54% for intermediate-risk prostate cancer.
- Progression-free survival (after salvage HIFU for local recurrence): 25-53%, depending on risk group.
- Cryotherapy: 7-year biochemical recurrence-free survival: 60% for low-risk patients, 48% for intermediate-risk patients.
- Radiation Therapy: 5-year survival after salvage radiation therapy (SRT): 72.5% progression-free survival for localized recurrent prostate cancer after HIFU.
Immunotherapy: for example Sipuleucel-T, has been shown to improve overall survival in advanced prostate cancer, especially in combination with conventional treatments.
Prostate Cancer Cure Rates Statistics
- Localized Prostate Cancer: 5-year biochemical disease-free survival is 97% in low-risk patients treated with radiation therapy or radical prostatectomy.
- Advanced Prostate Cancer: 5-year survival rate for metastatic prostate cancer is approximately 32.3%.
Post-Treatment Recurrence and Survival Statistics
- Prostatectomy: 5-year biochemical progression-free survival was 76% for localized prostate cancer.
- HIFU Recurrence Rate: 50-70% of patients remained free from biochemical recurrence 5 years after HIFU.
Prostate Cancer Death Rate Statistics
Prostate cancer continues to be a significant health issue globally, contributing to a considerable number of deaths among men. Here are the key statistics for 2022:
Global Prostate Cancer Deaths: According to the World Health Organization (WHO) and GLOBOCAN, prostate cancer was responsible for approximately 397,430 deaths worldwide in 2022, slightly increasing from 375,000 deaths reported in 2020. This positions prostate cancer as the fifth leading cause of cancer deaths among men globally.
Prostate Cancer Death Rate: Prostate cancer accounts for about 3.8% of all cancer deaths among men worldwide. This statistic underscores the substantial impact of the disease on male health.
Highest Mortality Rates: Certain regions experience significantly higher mortality rates from prostate cancer, particularly:
- Caribbean countries: These areas report some of the highest mortality rates due to factors such as limited access to healthcare and early detection.
- Sub-Saharan Africa: Similar challenges in healthcare access contribute to elevated mortality rates.
- Eastern Europe: Limited resources and healthcare infrastructure in some Eastern European countries lead to higher rates of prostate cancer deaths.
Lowest Mortality Rates: Conversely, countries with advanced healthcare systems report lower mortality rates from prostate cancer. Notable examples include:
- United States: Enhanced screening and treatment options result in a mortality rate of approximately 8.1 deaths per 100,000 men.
- Japan: Effective healthcare strategies contribute to lower mortality figures.
- Western Europe: Countries in this region benefit from comprehensive healthcare services, resulting in better survival outcomes.
Prostate Cancer Date Rate in the U.S.
- In the United States, the prostate cancer death rate is approximately 18.9 deaths per 100,000 men annually (as of the most recent data).
- In 2024, it is estimated that 35,250 men will die from prostate cancer, making it the second leading cause of cancer death in American men, behind lung cancer.
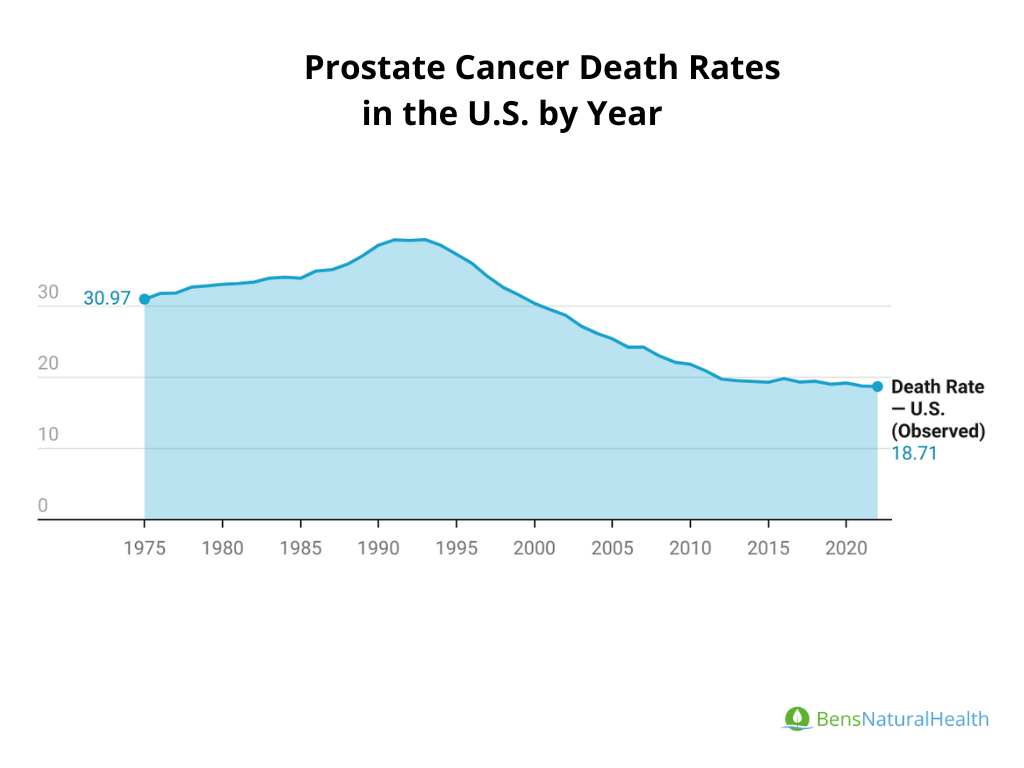
Trends in Prostate Cancer Mortality Rate: Prostate cancer death rates have declined substantially over the past few decades in developed countries like the U.S. due to improvements in early detection (e.g., PSA testing) and better treatments (e.g., surgery, radiation, hormone therapy).In the U.S., prostate cancer death rates have dropped by more than 50% since the early 1990s.
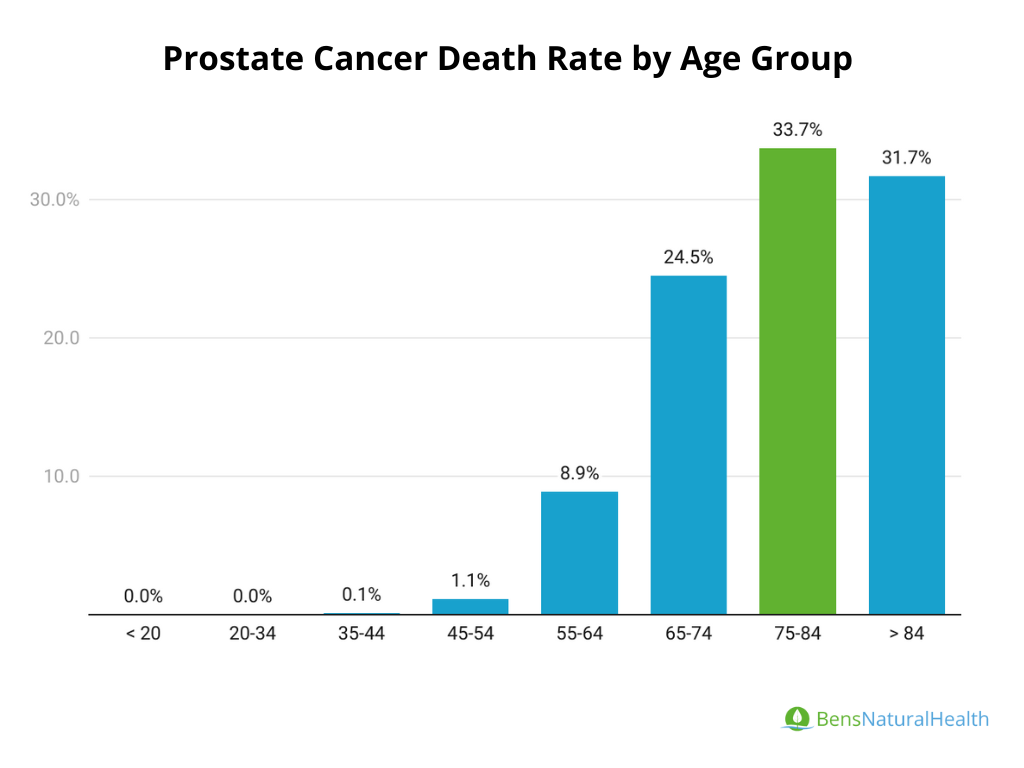
Prostate Cancer Mortality Rate by Age Group
Prostate cancer disproportionately affects older men, with the majority of deaths occurring in individuals aged 65 and older. As shown in the data, the risk of death increases significantly with age. The highest percentage of prostate cancer deaths occurs in men between the ages of 75 and 84
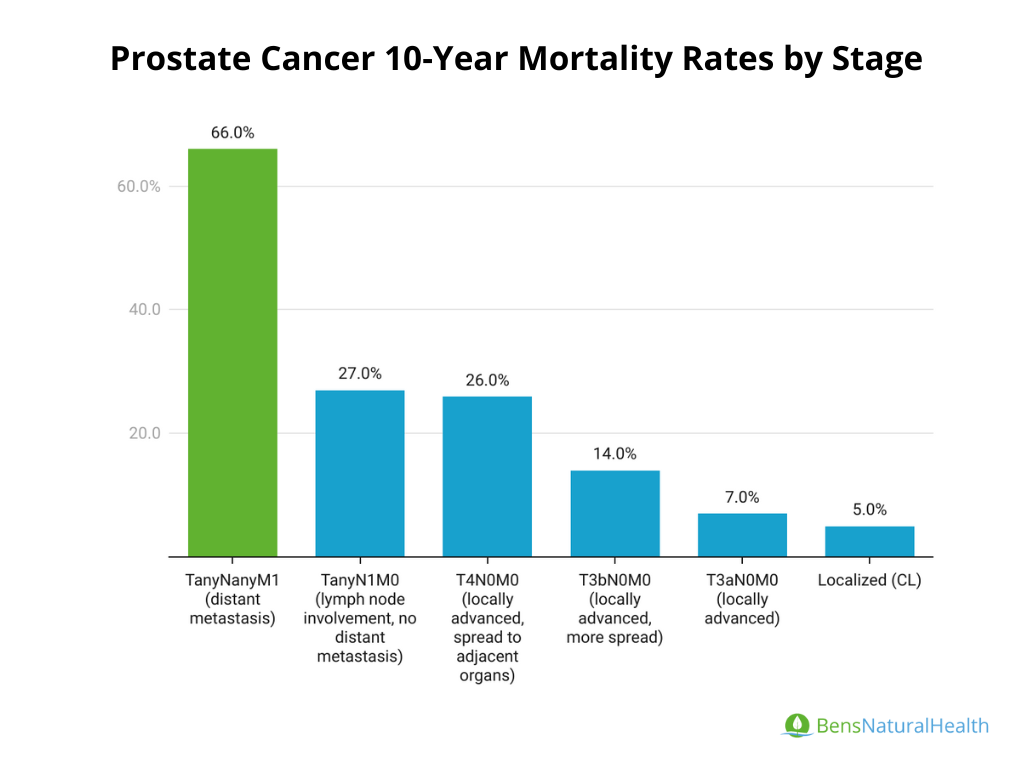
10-Year Prostate Cancer Mortality Rates by Stage
- Localized (CL): Cancer confined to the prostate: 5% mortality
- T3aN0M0 (locally advanced): Tumor has extended through the prostate capsule but has not spread to lymph nodes or distant sites: 7% mortality
- T3bN0M0 (locally advanced, more spread): Tumor has invaded the seminal vesicles, but has not spread to lymph nodes or distant sites: 14% mortality
- T4N0M0 (locally advanced, spread to adjacent organs): Tumor has spread to nearby organs (like the bladder or rectum) but not to lymph nodes or distant sites: 26% mortality
- TanyN1M0 (lymph node involvement, no distant metastasis): Tumor of any size with lymph node involvement but no distant metastasis: 27% mortality
- TanyNanyM1 (distant metastasis): Tumor of any size with lymph node involvement and distant metastasis (spread to other organs or bones): 66% mortality.
- T (Tumor): Indicates the size and extent of the main tumor.
- N (Nodes): Describes whether the cancer has spread to nearby lymph nodes.
- M (Metastasis): Refers to whether the cancer has spread to other body parts.
Ethnic and Racial Disparities in Mortality Statistics
If you’re wondering what ethnic group has a significantly higher incidence rate of prostate cancer, here are some important statistics to know:
- African American men (non-Hispanic Black) have the highest incidence of prostate cancer in the U.S. and globally. They are about 1.7 times more likely to develop prostate cancer compared to White men.
- Death Rate: African American men are also about 2 times more likely to die from prostate cancer compared to White men. Their death rate is approximately 37.2 deaths per 100,000, while the death rate for White men is around 18.1 per 100,000.
What Percent of Black Men Get Prostate Cancer?
- African American men have the highest lifetime risk of prostate cancer. About 1 in 6 Black men in the U.S. will be diagnosed with prostate cancer in their lifetime, compared to 1 in 8 for White men.
- There are known genetic differences that contribute to the higher incidence and mortality among African-American men, including higher rates of genetic mutations related to prostate cancer progression.
Other Racial and Ethnic Groups:
- Hispanic men: Tend to have lower prostate cancer incidence and mortality rates compared to African-American men but may show increased rates in certain regions.
Asian and Pacific Islanders: Have the lowest rates of prostate cancer incidence and mortality among all racial groups.
Prostate Cancer Recurrence Rate Statistics
The recurrence rate of prostate cancer depends on several factors, including the stage at diagnosis, type of treatment, and individual risk factors such as Gleason score and PSA levels. Recurrence is typically measured as a rise in PSA (prostate-specific antigen) levels after initial treatment, also known as biochemical recurrence.
- Surgery (Radical Prostatectomy):
- Recurrence Rate: Approximately 20-30% of men experience a biochemical recurrence within 10 years after surgery for localized prostate cancer.
- Factors Affecting Recurrence: Higher Gleason scores, positive surgical margins, and advanced stage at diagnosis increase the likelihood of recurrence.
- Radiation Therapy:
- Recurrence Rate: Similar to surgery, around 20-30% of men may experience a biochemical recurrence within 10 years.
- Factors Affecting Recurrence: PSA levels and tumor characteristics at diagnosis play a significant role in determining recurrence risk.
- Hormone Therapy (For Advanced Cancer):
- Hormone therapy is often used for advanced or metastatic prostate cancer. Over time, many cancers become resistant to hormone therapy (known as castration-resistant prostate cancer).
Progression to Castration-Resistant: Approximately 10-20% of men treated with hormone therapy develop castration-resistant prostate cancer within 3-5 years.
Healthcare Costs Statistics on Prostate Cancer
Prostate cancer treatment and management costs vary based on the stage at diagnosis, type of treatment, and long-term care needs. Here are general estimates for different stages and treatments in the U.S.
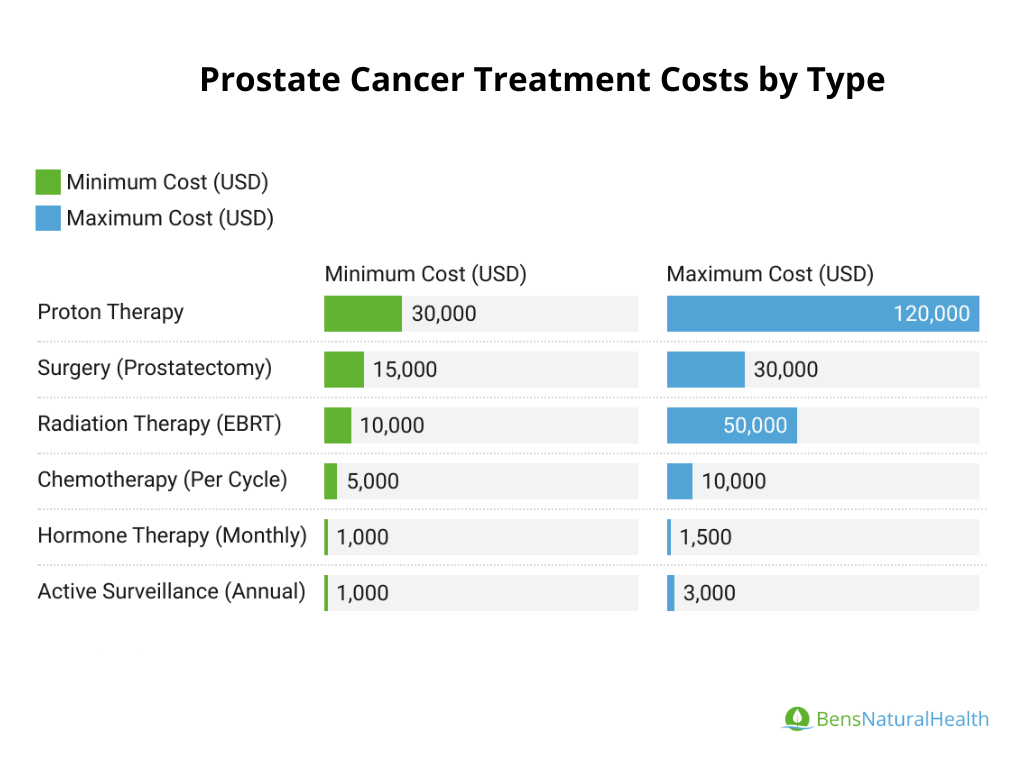
- Surgery (Prostatectomy):
Cost: The average cost of a radical prostatectomy ranges from $15,000 to $30,000.
Additional costs can occur for hospital stays, follow-up care, and management of side effects (e.g., incontinence, erectile dysfunction).
- Radiation Therapy:
External Beam Radiation Therapy (EBRT): Costs range from $10,000 to $50,000, depending on the number of sessions and type of radiation.
Proton Therapy: More expensive than traditional radiation, ranging from $30,000 to $120,000 for a full course of treatment.
- Hormone Therapy:
Cost: Hormone therapy, typically administered as injections, costs approximately $1,000 to $1,500 per month. Long-term use can make this treatment costly over time, particularly for advanced-stage cancer.
- Chemotherapy:
Cost: For metastatic prostate cancer, chemotherapy (e.g., docetaxel) costs about $5,000 to $10,000 per cycle, with a typical course involving 6 cycles.
- Active Surveillance:
Cost: Monitoring with regular PSA tests, biopsies, and imaging costs around $1,000 to $3,000 per year but avoids immediate treatment costs.
Total lifetime costs for localized (early stage) prostate cancer treatment (surgery or radiation) and follow-up can range from $25,000 to $60,000 over a lifetime. Total lifetime costs for advanced prostate cancer treatment can reach $100,000 to $200,000 or more, depending on the length of treatment and the need for ongoing therapies.
Global Predictions for Prostate Cancer Incidence and Mortality
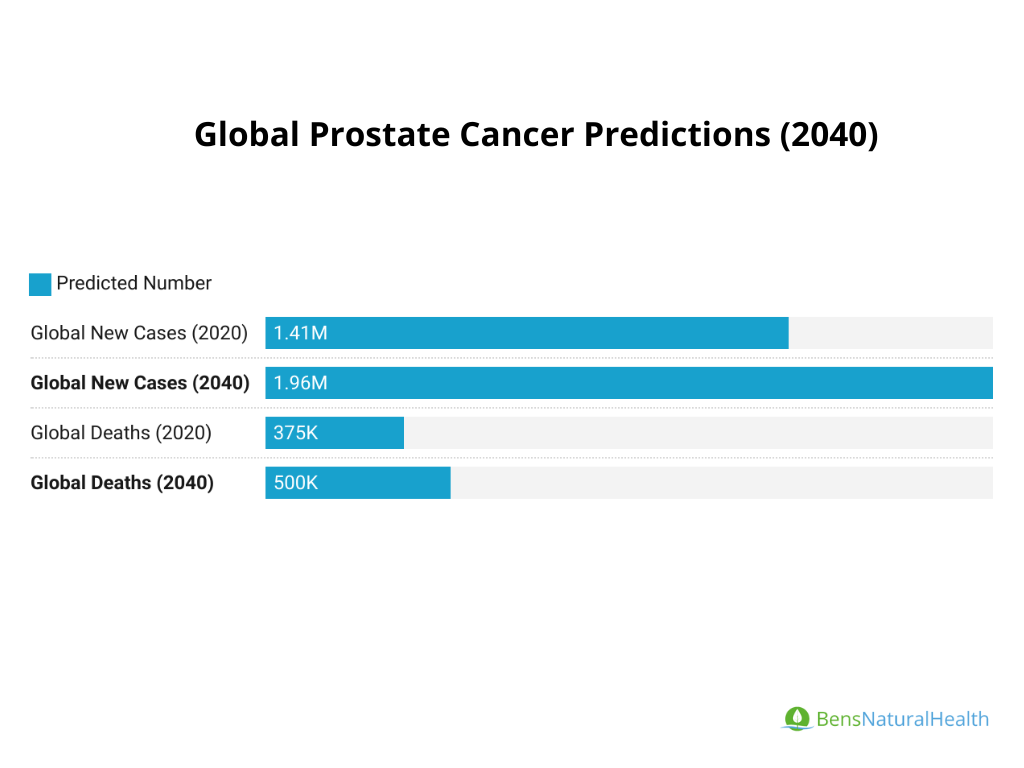
- Incidence: The global burden of prostate cancer is expected to rise in the coming decades due to aging populations and improved screening.
- By 2040, it is projected that there will be 1.96 million new cases of prostate cancer worldwide, a significant increase from the 1.41 million cases in 2020.
- By 2040, it is projected that there will be 1.96 million new cases of prostate cancer worldwide, a significant increase from the 1.41 million cases in 2020.
- Mortality: While death rates have been decreasing in high-income countries due to better treatments and early detection, prostate cancer mortality is expected to increase in low- and middle-income countries due to limited access to healthcare.
- Global prostate cancer deaths are projected to increase from 375,000 deaths in 2020 to over 500,000 deaths annually by 2040.
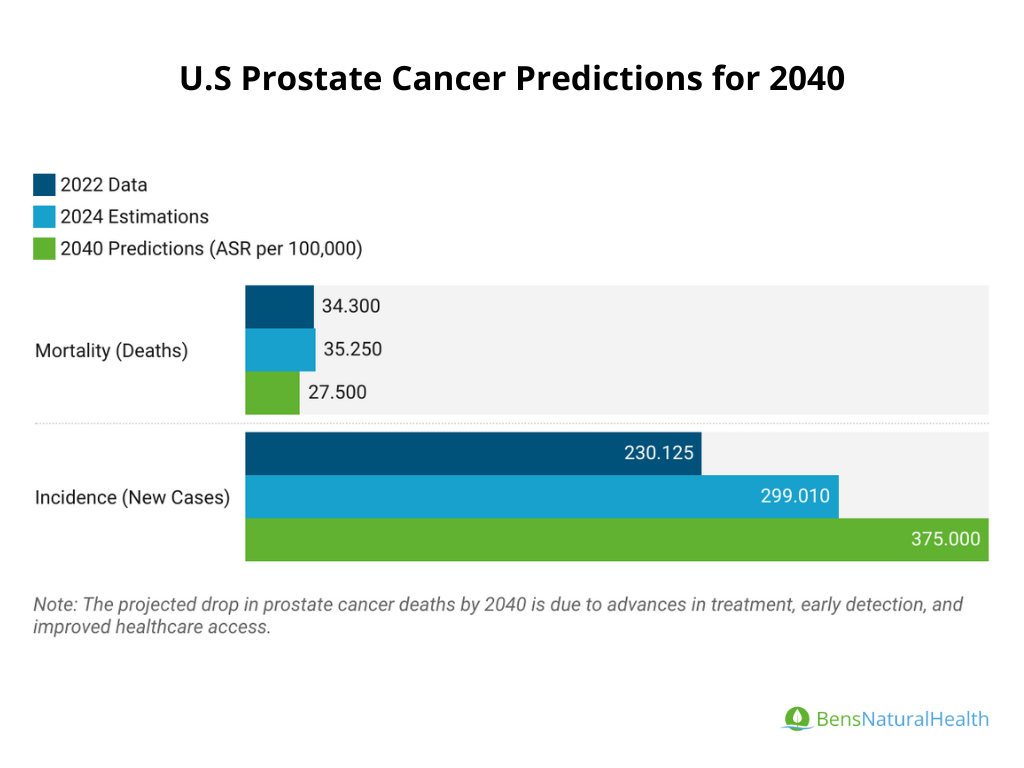
United States Prostate Cancer Predictions
- Incidence: In the U.S., prostate cancer remains the most common cancer in men, with 299,010 new cases expected in 2024. The incidence rate has remained relatively stable in recent years but could rise slightly with increased awareness and screening.
- Mortality: The death rate from prostate cancer in the U.S. has been steadily declining due to advances in early detection and treatment. In 2024, approximately 35,250 deaths from prostate cancer are expected. Continued improvements in treatment are projected to reduce mortality further, although challenges remain, particularly in high-risk groups (e.g., African American men).
Key Factors Impacting Future Projections
- Aging Population: As the global population ages, prostate cancer incidence will rise because it is primarily a disease of older men.
- Screening Practices: The use of PSA testing can lead to earlier detection, but screening guidelines may influence trends in diagnosis rates.
- Advances in Treatment: New treatments, including immunotherapy and targeted therapies, could further reduce mortality, particularly in advanced stages.
Research Methodology
- Data Collection: We gathered data from highly reputable and trustworthy sources, including:
- Surveillance, Epidemiology, and End Results (SEER) Program
- Global Cancer Observatory (GLOBOCAN)
- American Cancer Society (ACS)
- World Health Organization (WHO)
Additionally, we reviewed peer-reviewed research papers from leading journals, such as The Journal of Urology, CA: A Cancer Journal for Clinicians, and Frontiers in Public Health, to incorporate the most recent research findings on prostate cancer. Our focus was on the latest data from 2020–2024 to ensure relevance and accuracy.
- Data Analysis: We used various statistical methods to analyze the data, including descriptive statistics and survival analysis. We cross-checked data from multiple sources to ensure accuracy. We’ve considered key factors like healthcare access, screening practices, and regional differences to provide a global perspective on prostate cancer trends.
- Expert Review: The article was medically reviewed by experts to make sure that the statistics and interpretations align with current medical understanding. This expert input ensures that our findings are accurate and medically sound.
- Ethical Standards: All data was collected ethically, following strict guidelines. We used de-identified data from cancer registries and public databases, ensuring no personal information was included.
- Limitations: We recognize that some limitations exist, such as the potential for data lag from cancer registries and geographical differences in healthcare access, which can affect specific statistics.
Ongoing Review and Updates: We are committed to updating this article with the latest data. As new information becomes available, we will regularly review and update it, incorporating expert feedback to maintain accuracy.
Conclusion
Prostate cancer remains a significant health issue for men worldwide, particularly for those over the age of 60. The prostate cancer statistics and facts we’ve explored illustrate the importance of awareness, early detection, and understanding the risk factors associated with this disease. With advancements in research and treatment options, the outlook for many diagnosed with prostate cancer continues to improve.

This article is for informational purposes only and does not serve as medical advice. The details provided here are not a replacement for, and should never be depended upon as, professional medical advice. Always consult your physician regarding the potential risks and benefits of any treatment.
Dr. Alberto Parra
Head Diagnostic Medical Sonographer
Dr. Alberto Parra, General Practitioner and Medical Sonographer, specializes in ultrasound imaging and is passionate about empowering patients by providing accessible, accurate medical information.
Our Medical Review Process
At Ben’s Natural Health, we are committed to maintaining the highest standards of accuracy, transparency, and scientific integrity. Every piece of content is carefully developed by medical professionals and undergoes a thorough review every 12 to 24 months. This ensures that our information remains current, reliable, and rooted in credible, evidence-based research. We reference only peer-reviewed studies from reputable medical journals, providing full citations and direct links to enhance trust and confidence. Learn more about our medical review process and research standards.
Our Editorial Guidelines
For over 25 years, Ben’s Natural Health has been a trusted source of scientifically backed, reliable health information. Our editorial guidelines uphold the highest quality and integrity for every article we publish. Each piece is written by qualified experts and undergoes independent quality checks. We prioritize transparency by clearly displaying contributor credentials and biographies at the beginning of every article. Read more about our editorial standards.
Medical Disclaimer
The content on this blog is for informational purposes only and should not be considered a substitute for professional medical advice, diagnosis, or treatment. While our articles are authored and reviewed by licensed medical professionals, they may not address your specific health concerns. Always consult a qualified healthcare provider before making any medical decisions.
Article Sources
- Bray, F., Ferlay, J., Soerjomataram, I., Siegel, R. L., Torre, L. A., & Jemal, A. (2018). Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: a cancer journal for clinicians, 68(6), 394-424.
- Rawla, P. (2019). Epidemiology of prostate cancer. World journal of oncology, 10(2), 63.
- American Cancer Society (2021). Cancer Facts & Figures 2021. Available at https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2021/cancer-facts-and-figures-2021.pdf.
- National Institute of Cancer (2021). Cancer Stat Facts: Prostate Cancer. Available at https://seer.cancer.gov/statfacts/html/prost.html.
- Weiner, A. B., Matulewicz, R. S., Eggener, S. E., & Schaeffer, E. M. (2016). Increasing incidence of metastatic prostate cancer in the United States (2004–2013). Prostate cancer and prostatic diseases, 19(4), 395-397.
- Eggener, S. E., Scardino, P. T., Walsh, P. C., Han, M., Partin, A. W., Trock, B. J., … & Stephenson, A. J. (2011). Predicting 15-year prostate cancer specific mortality after radical prostatectomy. The Journal of urology, 185(3), 869-875.
- Cooperberg, M. R., Broering, J. M., & Carroll, P. R. (2009). Risk assessment for prostate cancer metastasis and mortality at the time of diagnosis. JNCI: Journal of the National Cancer Institute, 101(12), 878-887.
- Kenfield, S. A., Stampfer, M. J., Chan, J. M., & Giovannucci, E. (2011). Smoking and prostate cancer survival and recurrence. Jama, 305(24), 2548-2555.
- Johansson, J. E., Andrén, O., Andersson, S. O., Dickman, P. W., Holmberg, L., Magnuson, A., & Adami, H. O. (2004). Natural history of early, localized prostate cancer. Jama, 291(22), 2713-2719.
- Chen, S. L., Wang, S. C., Ho, C. J., Kao, Y. L., Hsieh, T. Y., Chen, W. J., … & Sung, W. W. (2017). Prostate cancer mortality-to-incidence ratios are associated with cancer care disparities in 35 countries. Scientific reports, 7(1), 1-6.
- Bleyer, A., Spreafico, F., & Barr, R. (2020). Prostate cancer in young men: An emerging young adult and older adolescent challenge. Cancer, 126(1), 46-57.
- O’Keefe, E. B., Meltzer, J. P., & Bethea, T. N. (2015). Health disparities and cancer: racial disparities in cancer mortality in the United States, 2000–2010. Frontiers in public health, 3, 51.
- Pernar, C. H., Ebot, E. M., Wilson, K. M., & Mucci, L. A. (2018). The epidemiology of prostate cancer. Cold Spring Harbor perspectives in medicine, 8(12), a030361.
- Barber, L., Gerke, T., Markt, S. C., Peisch, S. F., Wilson, K. M., Ahearn, T., … & Mucci, L. A. (2018). Family history of breast or prostate cancer and prostate cancer risk. Clinical Cancer Research, 24(23), 5910-5917.
- National Cancer Institue (NCI): https://seer.cancer.gov/statfacts/html/prost.html
- American Cancer Society (ACS): “Prostate Cancer Facts & Figures” – https://www.cancer.org
- World Health Organization (WHO) GLOBOCAN 2020: Global Cancer Statistics – https://gco.iarc.fr
- Centers for Disease Control and Prevention (CDC): Prostate Cancer Statistics – https://www.cdc.gov
- World Cancer Research Fund International: https://www.wcrf.org/
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021 May;71(3):209-249. doi: 10.3322/caac.21660. Epub 2021 Feb 4. PMID: 33538338.
- Wang, L., Lu, B., He, M., Wang, Y., Wang, Z., & Du, L. (2022). Prostate Cancer Incidence and Mortality: Global Status and Temporal Trends in 89 Countries From 2000 to 2019. Frontiers in Public Health, 10. https://doi.org/10.3389/fpubh.2022.811044.
- Teoh, J., Hirai, H., Ho, J., Chan, F., Tsoi, K., & Ng, C. (2019). Global incidence of prostate cancer in developing and developed countries with changing age structures. PLoS ONE, 14. https://doi.org/10.1371/journal.pone.0221775.
- Siegel, R., Miller, K., Fuchs, H., & Jemal, A. (2022). Cancer statistics, 2022. CA: A Cancer Journal for Clinicians, 72. https://doi.org/10.3322/caac.21708.
- Hinata, N., & Fujisawa, M. (2022). Racial Differences in Prostate Cancer Characteristics and Cancer-Specific Mortality: An Overview. The World Journal of Men’s Health, 40, 217 – 227. https://doi.org/10.5534/wjmh.210070.
- Bhardwaj, A., Srivastava, S., Khan, M., Prajapati, V., Singh, S., Carter, J., & Singh, A. (2017). Racial disparities in prostate cancer: a molecular perspective.. Frontiers in bioscience, 22, 772-782 . https://doi.org/10.2741/4515.
- Rebbeck, T. (2018). Prostate Cancer Disparities by Race and Ethnicity: From Nucleotide to Neighborhood.. Cold Spring Harbor perspectives in medicine, 8 9. https://doi.org/10.1101/cshperspect.a030387.
- Clark, R., Vesprini, D., & Narod, S. (2022). The Effect of Age on Prostate Cancer Survival. Cancers, 14. https://doi.org/10.3390/cancers14174149.
- Smith, C., Bauer, J., Connelly, R., Seay, T., Kane, C., Foley, J., Thrasher, J., Kusuda, L., & Moul, J. (2000). Prostate cancer in men age 50 years or younger: a review of the Department of Defense Center for Prostate Disease Research multicenter prostate cancer database.. The Journal of urology, 164 6, 1964-7 . https://doi.org/10.1016/S0022-5347(05)66929-7.
- Sun, L., Caire, A., Robertson, C., George, D., Polascik, T., Maloney, K., Walther, P., Stackhouse, D., Lack, B., Albala, D., & Moul, J. (2009). Men older than 70 years have higher risk prostate cancer and poorer survival in the early and late prostate specific antigen eras.. The Journal of urology, 182 5, 2242-8 . https://doi.org/10.1016/j.juro.2009.07.034.
- Slater, J., Rossi, C., Yonemoto, L., Bush, D., Jabola, B., Levy, R., Grove, R., Preston, W., & Slater, J. (2004). Proton therapy for prostate cancer: the initial Loma Linda University experience.. International journal of radiation oncology, biology, physics, 59 2, 348-52 . https://doi.org/10.1016/j.urolonc.2004.08.009.
- Tourinho-Barbosa, R., Sanchez-Salas, R., Claros, O., Collura-Merlier, S., Bakavičius, A., Carneiro, A., Stabile, A., Moschini, M., Cathala, N., Tobias-Machado, M., & Cathelineau, X. (2019). Focal Therapy for Localized Prostate Cancer with Either HIFU or Cryoablation: A Single Institution Experience.. Journal of Urology. https://doi.org/10.1097/JU.0000000000000506.
- Murat, F., Poissonnier, L., Rabilloud, M., Belot, A., Bouvier, R., Rouvière, O., Chapelon, J., & Gelet, A. (2009). Mid-term results demonstrate salvage high-intensity focused ultrasound (HIFU) as an effective and acceptably morbid salvage treatment option for locally radiorecurrent prostate cancer.. European urology, 55 3, 640-7 . https://doi.org/10.1016/j.eururo.2008.04.091.
- Boissier, R., Regis, F., Loverde, K., Territo, A., Toledano, H., Gallioli, A., Bastide, C., Rossi, D., Breda, A., & Palou, J. (2019). MP78-18 LONG TERM ONCOLOGICAL OUTCOMES OF CRYOABLATION AND HIFU IN WHOLE GLAND AND FIRST LINE TREATMENT FOR LOCALIZED PROSTATE CANCER. The Journal of Urology, 201, e1149–e1150. https://doi.org/10.1097/01.JU.0000557350.47574.a6.
- Riviere, J., Bernhard, J., Robert, G., Wallerand, H., Déti, E., Maurice-Tison, S., Ardiet, J., Maire, J., Richaud, P., Ferrière, J., Ballanger, P., Gelet, A., & Pasticier, G. (2010). Salvage radiotherapy after high-intensity focussed ultrasound for recurrent localised prostate cancer.. European urology, 58 4, 567-73 . https://doi.org/10.1016/j.eururo.2010.06.003.
- Liang, H., Liu, Y., Guo, J., Dou, M., Zhang, X., Hu, L., & Chen, J. (2023). Progression in immunotherapy for advanced prostate cancer. Frontiers in Oncology, 13. https://doi.org/10.3389/fonc.2023.1126752.
- Bryant, C., Smith, T., Henderson, R., Hoppe, B., Mendenhall, W., Nichols, R., Morris, C., Williams, C., Su, Z., Li, Z., Lee, D., & Mendenhall, N. (2016). Five-Year Biochemical Results, Toxicity, and Patient-Reported Quality of Life After Delivery of Dose-Escalated Image Guided Proton Therapy for Prostate Cancer.. International journal of radiation oncology, biology, physics, 95 1, 422-34 . https://doi.org/10.1016/j.ijrobp.2016.02.038.
- Siegel, D., O’Neil, M., Richards, T., Dowling, N., & Weir, H. (2020). Prostate Cancer Incidence and Survival, by Stage and Race/Ethnicity — United States, 2001–2017. Morbidity and Mortality Weekly Report, 69, 1473 – 1480. https://doi.org/10.15585/mmwr.mm6941a1.
- Amling, C., Blute, M., Bergstralh, E., Seay, T., Slezak, J., & Zincke, H. (2000). Long-term hazard of progression after radical prostatectomy for clinically localized prostate cancer: continued risk of biochemical failure after 5 years.. The Journal of urology, 164 1, 101-5 . https://doi.org/10.1016/S0022-5347(05)67457-5.
- Brenner, H., & Arndt, V. (2005). Long-term survival rates of patients with prostate cancer in the prostate-specific antigen screening era: population-based estimates for the year 2000 by period analysis.. Journal of clinical oncology : official journal of the American Society of Clinical Oncology, 23 3, 441-7 . https://doi.org/10.1200/JCO.2005.11.148.
- Aliakbari, F., Ghanbari, M., Khayamzadeh, M., Hajian, M., Allameh, F., Ahadi, M., Sadeghzadeh, Z., Akbari, M., Solimani, M., & Nematollah, S. (2020). Five-year Survival Rate of Prostate Cancer in Iran: Results of the national cancer-registry system during 2010-2015. , 4. https://doi.org/10.22037/MHJ.V4I1.30451.
- Critz, F., & Levinson, K. (2004). 10-year disease-free survival rates after simultaneous irradiation for prostate cancer with a focus on calculation methodology.. The Journal of urology, 172 6 Pt 1, 2232-8 . https://doi.org/10.1097/01.JU.0000144033.61661.31.
- Shukla, M., Yu, C., Reddy, C., Stephans, K., Klein, E., Abdel-Wahab, M., Ciezki, J., & Tendulkar, R. (2015). Evaluation of the current prostate cancer staging system based on cancer-specific mortality in the surveillance, epidemiology, and end results database.. Clinical genitourinary cancer, 13 1, 17-21 . https://doi.org/10.1016/j.clgc.2014.07.003.
- Albertsen, P., Hanley, J., & Fine, J. (2005). 20-year outcomes following conservative management of clinically localized prostate cancer.. JAMA, 293 17, 2095-101 . https://doi.org/10.1016/J.UROLONC.2005.08.017.
Article Update History
Updated on 29 January, 2025 (Current Version)
Created on 11 April, 2021
Explore More
New Guidelines On Prostate Cancer Screening For Black Men
The goal of prostate cancer screening is to detect it early and find it before it spreads and causes symptoms. Late detection can lead ...