When to Take Insulin for Type 2 Diabetes


Article Summary
- Many people with type 2 diabetes will end up being treated with injectable insulin to meet their blood sugar targets.
- There are many kinds of insulin available, which can help to tailor a customized insulin regimen to a person’s health and lifestyle needs.
- The benefits of insulin injections are improved blood sugar levels, reduced risk of diabetes-related complications, and decreased pancreatic strain.
Diabetes mellitus, or diabetes, is a disease affecting blood glucose (sugar) levels.
An organ called the pancreas creates the hormone insulin, which helps keep blood sugar levels in a healthy range.
With diabetes, the pancreas either doesn’t make enough insulin, or the body doesn’t respond to it well. Without proper insulin function, blood sugar levels rise and can lead to health problems if left untreated.
Diabetes is becoming more prevalent worldwide. As of 2015, 30.3 million people in the United States, or about 9.4 percent of the population, had diabetes. Unfortunately, more than one in four people with diabetes don’t know they have it. Having undiagnosed diabetes increases the risk of complications from lack of prompt treatment.
Many people also have prediabetes, a condition where blood sugars are slightly elevated but not high enough to be considered diabetes. Having prediabetes is a significant risk factor for eventually developing type 2 diabetes.
The U.S. Centers for Disease Control (CDC) estimates that up to 30% of people with prediabetes will develop type 2 diabetes within five years of their prediabetes diagnosis.
The majority of people with diabetes have type 2 diabetes, which usually results from insulin resistance and a combination of several risk factors.
Some of the most common risk factors for type 2 diabetes include:
- Weight: People who are considered overweight or obese according to their body mass index (BMI).
- Age: people 45 and older are at increased risk.
- Family history of diabetes
- Race/ethnicity: diabetes tends to affect certain races more than others. At-risk races include African American, Alaska Native, Native American, Asian American, Hispanic/Latino, Native Hawaiian, or Pacific Islander.
- High blood pressure: if your blood pressure is higher than 120/80, you may be at increased risk.
- Altered lipid levels: low levels of HDL “good” cholesterol and high levels of LDL “bad” cholesterol are risk factors, as well as high triglycerides (blood fat).
- Pregnancy history: women with a history of gestational diabetes (GDM) or who gave birth to a baby 9 pounds or heavier are at increased risk.
- Physical activity: People who aren’t regularly active or who have a sedentary lifestyle are at increased risk.
- Smoking status: Smokers are 30-40% more likely to develop type 2 diabetes than nonsmokers.
- Health history: those with a history of heart attack or stroke have a higher likelihood of developing type 2 diabetes.
- PCOS: Polycystic Ovarian Syndrome in women is a risk factor, as it usually is associated with insulin resistance.
- Acanthosis nigricans: dark, velvety patches of skin are a sign of insulin resistance and are a risk factor for developing diabetes. These patches of skin usually occur around the neck or armpits.
Type 1 diabetes is an autoimmune condition and is rarer than type 2 diabetes. Type 1 diabetes results from the body attacking the cells in the pancreas responsible for producing insulin. People with type 1 diabetes need to take insulin to manage their diabetes, whereas people with type 2 diabetes don’t always have to take insulin.
There are several medication options for people with type 2 diabetes that don’t involve injecting insulin. Some of the medications available for type 2 diabetes are:
- Metformin: Helps to reduce the amount of sugar released by the liver and improves insulin sensitivity
- Sulfonylureas: Stimulate the pancreas to secrete more insulin
- GLP-1 receptor agonists: Promote insulin production, decrease glucose release from the liver, and slows stomach emptying to increase satiety
- DPP-4 inhibitors: Promote insulin production, decrease glucagon (a hormone that increases blood sugar) production and delays gastric emptying
People with type 2 diabetes may need to end up taking insulin at some point. Needing to take insulin doesn’t mean that these individuals failed at managing their blood sugars without insulin; over time, the pancreas can lose its ability to produce enough insulin to support healthy blood sugar levels.
This can occur due to a combination of insulin resistance and pancreatic insufficiency from years of trying to produce insulin to combat high blood sugar levels. People with a long history of diabetes are more likely to need insulin therapy than those recently diagnosed.
Types of insulin
There are many different types of insulin available. Combining different insulin types can create a customized insulin regimen to meet the needs of people’s individual blood sugar trends and targets.
Insulin is described by its onset, peak, and duration. Onset refers to how quickly after injection the insulin starts working to lower blood sugars. Peak refers to the time when the insulin is working the hardest to lower blood sugar and is reported in terms of time elapsed after injection.
Duration refers to how long the insulin has effects on blood sugar or how long it lasts. Insulin with short onset and peak tends to lower blood sugar levels more quickly, while insulin with a more delayed onset and peak tends to work more slowly to lower blood sugar levels.
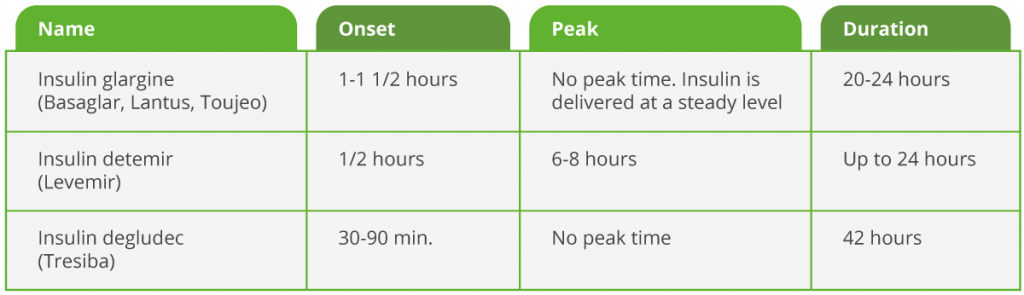
Basal insulin, or “background” insulin, mimics the pancreas’ slow-releasing insulin throughout the day and night. It’s also called long-acting insulin. Basal insulin helps counteract the glucose released by the liver and helps to control blood sugar between meals. People usually inject basal insulin once or twice daily, typically in the morning and at bedtime. It can be taken alone or combined with shorter-acting insulins at mealtimes.
Basal insulin usually has little to no peak and a long duration. Below are some common types of basal insulin available today:
Short-acting insulin has an onset of 30-60 minutes and peaks around 2-5 hours after injecting. Novolin, or “regular” insulin, is short-acting insulin and was the most common type of mealtime (also called prandial or bolus) insulin before the rapid-acting insulins were developed. Short-acting insulin is appropriate for taking within 30-60 minutes of a meal.
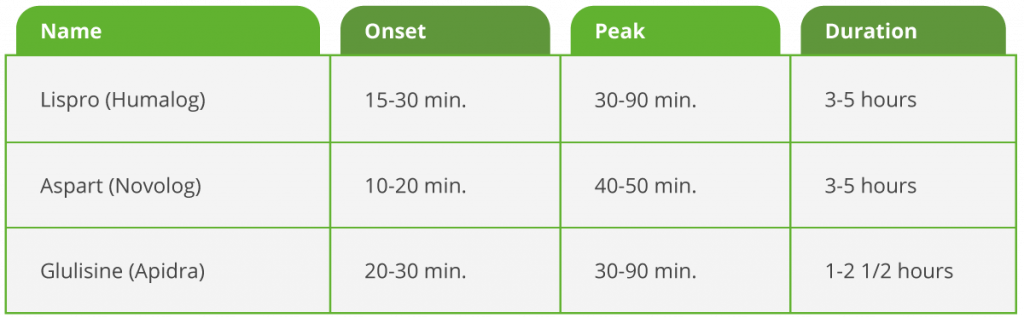
Rapid-acting insulins work the quickest to lower blood sugar and are used to cover insulin needs at mealtime. These insulins work to mimic how a pancreas without diabetes will release a larger amount of insulin at once when blood sugar levels start to rise after a meal. Because of their quick onset (under 30 minutes) and peak (less than 90 minutes), they should be taken when starting a meal, unlike regular insulin, which can be taken 30-60 minutes before a meal. Below are the rapid-acting insulins used today:
Intermediate-acting insulin has an onset of 1-2 hours and peaks around 4-12 hours after injecting. It helps cover insulin needs for about half of the day, so it is often used twice daily to provide full-day insulin coverage. NPH can be mixed with shorter-acting insulins. Humulin N and Novolin N are both brand names of NPH insulin.
Premixed insulins combine intermediate-acting insulin (NPH) with rapid- or short-acting insulin. This creates varied times of onset, peak, and duration. The first number in the name correlates with how much of the combination is intermediate-acting. The second number is how much of the combination is short- or rapid-acting insulin. For example, Humulin 70/30 is 70% NPH insulin and 30% regular (short-acting) insulin, and Humulin 50/50 is 50% NPH insulin and 50% regular insulin. The premixed insulins available today include:

Pens versus vials: Insulin is available in both vials and pens. Insulin in vials must be drawn up into a separate syringe and then injected, which means there is more room for user error. Air bubbles can also impact the accuracy of insulin injections when using a vial.
Insulin pens are more compact and require a new needle to be attached to each injection pen. The correct insulin dose can be achieved by turning a dial until the correct dose appears in the display window. This option is often safer for people with poor vision, limited dexterity, or those who simply want a more convenient type of insulin.
Benefits of insulin injections
- Effective at lowering blood sugar. Injecting insulin is the best way to mimic the pancreas’ normal ability to produce enough insulin to control blood sugar levels. Other medications can stimulate the pancreas to release insulin, but it might not be enough to manage high blood sugars.
- Eases the burden on the pancreas. When blood sugars are high, the pancreas works harder to produce enough insulin to lower glucose levels. This can strain the pancreas and cause pancreatic insufficiency and higher blood sugars. Injecting insulin helps ease this burden and may help the pancreas regain some of its function or help prevent further damage to the pancreas.
- Reduce the risk of diabetes complications. Many people with diabetes experience improved blood sugar levels after starting an insulin regimen. Improved blood sugar control helps to prevent diabetes-related complications from chronic uncontrolled blood sugar.
Disadvantages of insulin injections
- Increased risk of low blood sugar. Hypoglycemia is the term for low blood sugar, which occurs when blood glucose falls below 70 mg/dL. Taking insulin increases the risk of hypoglycemia, especially when insulin isn’t taken as prescribed or a meal is missed, among other reasons. Low blood sugar can become life-threatening if severe, making proper insulin dosing and follow-up with a healthcare provider critical for the safety of the patient.
- Fear of needles. One of the major concerns among people contemplating starting insulin is their fear of needles. This fear generally goes away quickly after the individual gets comfortable injecting their insulin the first few times. Needles for injecting insulin come in very fine sizes, which helps reduce the pain of injections.
- Need for proper storage. Insulin can go bad if it’s stored improperly, such as being left in the heat or cold too long.
- Weight gain. Improved blood sugar levels from taking insulin can result in weight gain. Insulin helps lower blood sugar levels but is also a fat-storage hormone, meaning that weight gain can be a side effect. When there isn’t enough insulin present and blood sugar levels climb, the body will burn fat stores for energy instead, resulting in weight loss (often a symptom of undiagnosed diabetes). Once blood sugar is improved through insulin use, these fat stores are no longer needed to provide energy, resulting in weight gain.
- Restrictions for some truck drivers. Some states have strict laws about truck drivers taking insulin because of the risk of hypoglycemia.
- Pain at the injection site. Most people don’t experience any issues when injecting insulin. However, some people may experience some skin discomfort, especially if they inject into the same area without rotating sites.
How much insulin will I need to take each day?
The amount of insulin injections required will vary depending on the individual, their blood sugar trends, and their blood sugar goals. Some people might take basal insulin once or twice daily, while others might take basal insulin twice daily and three mealtime insulin doses per day.
Healthcare providers typically start with basal insulin and titrate it (adjust it) based on how the patient’s blood sugars respond to the dose. Insulin doses are defined in terms of units. The American Diabetes Association recommends starting at 10 units of insulin, or 0.1-0.2 units of insulin per kilogram, and adjusting it by 10-15% or 2-4 units twice weekly until fasting blood sugar targets are met.
If blood sugar targets still aren’t met with basal insulin therapy, then adding mealtime insulin before the largest meal of the day is the next recommended step. If blood sugar targets still aren’t being met after that, then taking mealtime insulin with other meals is the next step. Here is a helpful visual of an algorithm developed to determine insulin dosages.
Ideally, 50% of the total dose of insulin would be basal, and 50% would be bolus (mealtime) insulin. However, some people are only on basal insulin because they’re at high risk for hypoglycemia or because their blood sugar levels are controlled with only basal insulin.
Prandial, or mealtime insulin, is usually adjusted based on pre-and post-meal blood sugars. For instance, if pre-lunch blood sugars aren’t usually very high, then the pre-breakfast dose is likely a target. However, if pre-lunch blood sugars are high, the breakfast prandial dose may need to be increased to help bring blood sugar levels to target before lunch.
A total daily dose of 200 units, or going above 2 units of insulin per kilogram of body weight per day, is generally considered to be a high amount. If a patient isn’t achieving blood sugar targets despite high doses of insulin, other steps need to be taken to address the insulin resistance.
When should you take insulin?
When to initiate insulin: Insulin is typically indicated when the hemoglobin A1c is greater than 9% or when other medications have failed to result in blood sugar targets.
Healthcare providers will prescribe insulin if the benefits outweigh the risks. For instance, elderly people living on their own can be at higher risk of hypoglycemia and might not have the mental clarity or dexterity to inject insulin and monitor blood sugar levels, making them a poor candidate for intensive insulin therapy.
What time of day to take insulin: Basal insulin is usually administered once or twice daily, upon waking and/or at bedtime. Intermediate-acting insulin (NPH) can also be taken twice a day, similar to basal insulin.
Mealtime insulin is to be taken prior to meals. With rapid-acting insulin, it’s best to inject the insulin right when starting a meal because it works so quickly. If it was injected, but the meal was somehow delayed or missed, hypoglycemia could result. On the other hand, short-acting insulin can be taken 30-60 minutes before a meal because it has a slower onset than rapid-acting insulin.
Where should you inject insulin?
Insulin is meant to be injected into the subcutaneous or fat tissue. The most preferred location is the abdomen, avoiding the skin within two inches of the belly button. Insulin is absorbed the most consistently in the abdominal area.
For people who have little fat on their abdomen, the upper thigh and/or upper arm can be used as alternative injection sites. The buttocks can also be utilized as an injection site, but it can be more difficult to self-administer insulin in the buttocks. Insulin shouldn’t be injected into the muscle.
Development in insulin injections
Ultra-long acting insulins, such as insulin glargine U300 (brand name Toujeo), are more concentrated than regular strength insulin. Most insulin contains 100 units per milliliter (U100), whereas U300 insulin has 300 units per milliliter. This means people requiring large amounts of insulin can take a lower volume of insulin without lowering the actual units of insulin taken.
Insulin degludec (brand name Tresiba) is a newer type of basal insulin, but it lasts longer than traditional basal insulins such as Lantus and Levemir. Longer-acting insulins may help reduce hypoglycemia risk.
Those wanting insulin that doesn’t require an injection is in luck! The FDA approved an inhaled version of rapid-acting insulin called Afrezza in 2014. It’s inhaled, similar to how asthma sufferers use an inhaler to deliver their asthma medication.
Conclusion
Many people with type 2 diabetes will end up being treated with injectable insulin to meet their blood sugar targets. There are many kinds of insulin available, which can help to tailor a customized insulin regimen to a person’s health and lifestyle needs.
Short- and rapid-acting insulins start to work within less than an hour to an hour and help to control blood sugar at mealtimes. This type of insulin is called bolus, prandial, or mealtime insulin. Basal insulin is longer-acting and is usually injected once or twice daily. Intermediate-acting insulin (NPH) falls between short- and long-acting and is usually injected twice daily or mixed with other insulin as a premixed injection.
The benefits of insulin injections are improved blood sugar levels, reduced risk of diabetes-related complications, and decreased pancreatic strain. The risks and side-effects of injecting insulin are low blood sugar, weight gain, and the fact that not everyone can follow an insulin regimen. Healthcare providers prescribe insulin when they feel the benefits outweigh the risks.
This article is for informational purposes only and does not serve as medical advice. The details provided here are not a replacement for, and should never be depended upon as, professional medical advice. Always consult your physician regarding the potential risks and benefits of any treatment.
Our Medical Review Process
At Ben’s Natural Health, we are committed to maintaining the highest standards of accuracy, transparency, and scientific integrity. Every piece of content is carefully developed by medical professionals and undergoes a thorough review every 12 to 24 months. This ensures that our information remains current, reliable, and rooted in credible, evidence-based research. We reference only peer-reviewed studies from reputable medical journals, providing full citations and direct links to enhance trust and confidence. Learn more about our medical review process and research standards.
Our Editorial Guidelines
For over 25 years, Ben’s Natural Health has been a trusted source of scientifically backed, reliable health information. Our editorial guidelines uphold the highest quality and integrity for every article we publish. Each piece is written by qualified experts and undergoes independent quality checks. We prioritize transparency by clearly displaying contributor credentials and biographies at the beginning of every article. Read more about our editorial standards.
Medical Disclaimer
The content on this blog is for informational purposes only and should not be considered a substitute for professional medical advice, diagnosis, or treatment. While our articles are authored and reviewed by licensed medical professionals, they may not address your specific health concerns. Always consult a qualified healthcare provider before making any medical decisions.
Article Sources
- https://www.niddk.nih.gov/health-information/diabetes/overview/what-is-diabetes
- https://www.tresibapro.com/content/tresibapro/en/dosing-and-administration/starting-adult-patients.html
- https://www.aafp.org/afp/2011/0715/p183.html
- https://www.ihs.gov/sites/diabetes/themes/responsive2017/display_objects/documents/algorithms/AlgorithmInsulinTherapy.pdf
- https://www.uptodate.com/contents/dipeptidyl-peptidase-4-dpp-4-inhibitors-for-the-treatment-of-type-2-diabetes-mellitus
- Sola D, Rossi L, Schianca GP, et al. Sulfonylureas and their use in clinical practice. Arch Med Sci. 2015;11(4):840-848. doi:10.5114/aoms.2015.53304
Article Update History
Updated on 25 July, 2026 (Current Version)
Created on 11 February, 2021
Explore More

Insulin Overdose: What To Do If You Take Too Much Insulin
Insulin is a vital hormone used to regulate blood sugar (glucose) in the body; however, taking too much insulin can be dangerous. Insulin is ...