Treatment Options for BPH: What Is a Prostatic Stent?


Article Summary
- A prostatic stent is a device that opens the male urethra permanently or temporarily.
- The device is specifically designed to be positioned into the urethra and bladder neck.
- Since the stent keeps the urethra open, it improves the flow of urine.
Benign prostatic hyperplasia (BPH), or enlarged prostate, is a common condition in men.
Prostate enlargement happens when the cells of the prostate gland start multiplying. The additional cells cause swelling of the almond-shaped gland. As the prostate swells, it squeezes the urethra and limits the urine flow.
The enlarged prostate affects the quality of life of about one-third of men older than 50 years.
The condition is present in up to 90% of men by the age of 85. Additionally, about 14 million men in the United States display BPH symptoms. On a global scale, 30 million men have this problem.
Symptoms of prostatic hyperplasia include:
- Difficulty starting urination
- Dribbling at the end of urinating
- Failing to empty the bladder completely
- Frequent need to urinate
- Nocturia (frequent need to urinate during the night)
- Urine stream stops and starts
- Weak urine stream
Even though prostate enlargement is uncomfortable and affects a man’s quality of life, patients can recover successfully. Various treatment options are available to help BPH. One of those options is a prostatic stent. In this post, we are going to shed more light on the prostatic stent and everything you need to know about it.
What is a prostatic stent?
Chances are the term stent that is familiar to you. That’s because the stent is such a frequent treatment option for various health problems. A stent is a tiny tube that a doctor inserts into a blocked passageway to keep it open.
The primary purpose of the stent is to restore the flow of blood or other fluids. Both metal and plastic stents are available. Stents are used for different health concerns, especially heart diseases. But they can also serve to address benign prostatic obstruction.
The stent may help manage and relieve bladder outlet obstruction to improve a patient’s quality of life. Besides benign prostatic hypertrophy, these devices may treat other prostate-related problems. Other uses of these devices require more research.
The question arises – what is a prostatic stent?
Also known as a prostate stent, a prostatic stent is a device that opens the male urethra permanently or temporarily. The device is specifically designed to be positioned into the urethra and bladder neck. Since the stent keeps the urethra open, it improves the flow of urine.
Generally speaking, stents are most suitable for men who are not eligible or fit for surgery but can still empty the bladder on their own.
For example, elderly men with acute urinary retention who are in poor overall health and unable to undergo more aggressive BPH treatments may benefit from the prostatic stent. These aggressive BPH treatments options include transurethral resection of the prostate (TURP). Prostatic stents are used instead of an indwelling catheter.
The purpose of a prostatic stent
The main premise behind the use of a cylinder-shaped device in the treatment of BPH is to preserve the luminal patency of hollow structures. This tiny, spring-like device pushes back the surrounding prostate tissue to widen the urethra.
Prostate stents are not a long-term solution, in most cases. For some men, they may not work. The success rate ranges from 50% to 90% of figures show, depending on the prostatic stent type. Yes, there are more of them! Some men may experience complications after undergoing this procedure.
The use of stents in the treatment of BPH is not a novel approach. Prostatic stents have been used since 1980. Over time, they have evolved significantly. Nowadays, different materials are available. The degree of urothelial reaction generated along with the shape of stents has also improved. As the prostate stents evolve, the degree of complications can decrease.
Benefits
Thanks to their potential to improve BPH symptoms, these devices may prevent complications such as bladder stones and other more serious consequences.
However, prostatic stenting in the United States became an option for BPH treatment later than elsewhere. Why? It’s primarily because of the strict regulatory forces governing the use of these devices. Prostate stenting is a minimally-invasive procedure with important benefits, such as:
- It’s fast
- Easy to perform
- Immediately effective
- More cost-effective than other approaches
How is a stent inserted?
As seen above, stent placement is a minimally-invasive procedure. The term minimally-invasive indicates the procedure doesn’t cause harm to the surrounding tissue. Also, it doesn’t require such a long recovery, like other procedures.
The whole concept of prostatic stents is simple.
The surgeon places a stent inside the prostate gland via an instrument called a flexible cystoscope. A flexible cystoscope is an instrument that can look inside a patient’s body. The stent is at the end of this instrument. Then, the surgeon carefully inserts it.
A patient is conscious during the procedure. This is typical for minimally-invasive surgeries. Don’t worry; you won’t feel anything thanks to local anesthesia. Basically, to make the procedure more effective, the surgeon applies local anesthetic jelly in the urethra. Then, a flexible cystoscope passes through the urethra and reaches the prostate.
When that happens, it’s time to position the stent. Since the flexible cystoscope features a small camera, the surgeon observes everything on the monitor. The procedure lasts 15 minutes on average.
Advantages and disadvantages to permanent prostatic stents
Although prostate stents are meant to be a temporary treatment for BPH, they can be permanent too. Various prostate stents are available nowadays. Epithelializing stents (or permanent prostatic stent) are devices that promote epithelialization and become embedded in the urethra.
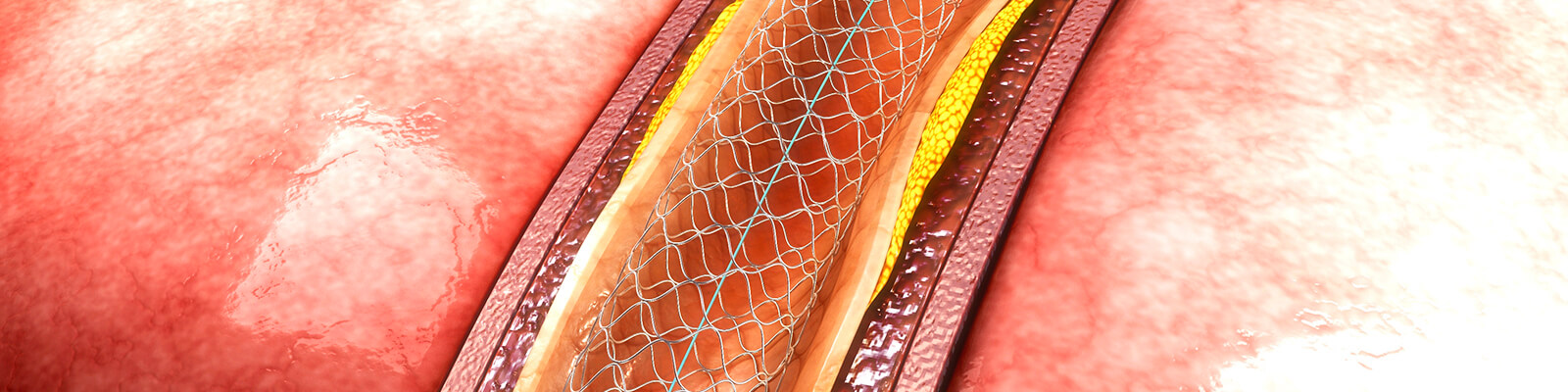
The first permanent stent was Urolume Wallstent, which contained stainless steel superalloy wire woven in a tubular mesh. This woven construction allows the ingrowth of urothelial tissue. The complete epithelization occurs within six to 12 months.
Besides Urolume stent, other devices of this kind include Memokath, a nonepithelializing stent designed for long-term use. Studies show when removal of these stents is necessary, the design of Memokath makes it easier to remove the device compared to Urolume.
What the research says
Initial studies with Urolume demonstrated encouraging results. But a long-term study from the BJU International weakened the optimism regarding these devices. The scientists evaluated 15 patients before they received a stent, after the procedure, and 10.5 years later. Of 15 subjects, only two men were satisfied with their stent.
Two failures occurred to excessive tissue proliferation in the stent, which led to the removal of the device. Then, two stents were removed due to pain and discomfort. Two subjects developed stenosis in the stent after seven and nine years, respectively. Common symptoms recorded at the last follow-up were lower urinary tract infection, urge and stress incontinence, and ejaculation discomfort. When it comes to ejaculatory problems, it’s useful to mention that many men with this health problem also experience retrograde ejaculation.
The same journal published a study that evaluated the 12-year outcome of Urolume prostate stent. The scientists followed 62 patients with moderate to severe lower urinary tract symptoms secondary to BPH. Patients received Urolume stent; one surgeon performed all procedures. The subjects were followed up at 12 weeks and six months after the procedure. Then, follow-ups occurred yearly for 12 years. Throughout the course of the study, scientists evaluated data such as symptom scoring, peak urinary flow rate (PFR), and postvoid residual volume (PVR).
At the end of the follow-up period, only 18% of the patients had the stent in place. Stent removal happened in 40% of subjects due to irritation symptoms, malpositioning, and dislodgement. The scientists concluded that Urolume is a safe treatment for BPH in select patients. Careful case selection and experience of the surgeon are crucial and mandatory.
A lot more studies are necessary to understand the long-term effectiveness of permanent prostatic stents. But, let’s focus on the advantages and disadvantages of these devices.
Advantages of permanent prostate stents
- Minimal bleeding during and after the procedure
- Quick procedure (15 minutes on average), local anesthesia
- Usually doesn’t require spending the night in the hospital; patients can go home the same day
Disadvantages of permanent prostate stents include:
- Due to fixed diameter, they may limit subsequent endoscopic surgical options
- May become dislodged, leading to total incontinence or urinary obstruction
- Mild discomfort
- Risk of increased urination and limited incontinence
- Risk of infections that may make removal more difficult
Advantages and disadvantages to temporary prostatic stents
The temporary or nonepithelializing prostatic stents have a number of advantages compared to the permanent spiral coils. They are expandable and also made of metal.
However, these stents are inserted in their compressed states with the delivery system. As a result, the risk of urethral injury is lower. The stent insertion process is better tolerated and may alleviate the prostatic obstruction. They may be a more practical alternative to the urinary catheter, a common approach today.
Not all temporary prostatic stents are the same. There are multiple generations of these devices, such as:
First-generation
The most notable representative is the Urospiral prostatic urethral stent made of coiled rust-proof stainless steel of fixed caliber. Even though early results were promising, the explantation rates were up to 40%. This was due to migration and the encrustation of the stent lumen. Another representative of first-generation prostate stents was Prostakah.
Second generation
Devices are newer, and materials are more biocompatible, e.g., nitinol. Biocompatible materials prevent encrustation. To prevent migration, second-generation prostatic stents are expandable. Well-known representatives of second-generation prostate stents include Prostacoil stent. Prostacoil stent was self-expanding and could be implanted under fluoroscopic guidance and local anesthesia. Compared to Prostakah, Prostacoil stent has more advantages, including a larger caliber that allows for more flexibility and longer indwelling time.
Third generation
Thermoexpandable stents such as Memokath stent. As mentioned earlier in this post, Memokath stent is in the group of temporary devices, but it is designed for long-term use. Memokath is a nickel-titanium alloy stent. When inserted in the correct place, the surgeon flushes the sent with heated water (55-65°C). Then, the stent expands and anchors in the right place. With refrigerator-cold irrigation fluid, the stent softens and uncoils into a nontraumatic wire, which is easy to remove. Evidence shows that Memokath stent is a safe, cost-effective, and potentially under-utilized treatment option. However, some studies found high migration rates were a major limitation of Memokath stents. While the stent led to the relief of outflow obstruction and improvement of symptom scores, it still migrated in 93% of cases. This stent may also work for bulbar urethral strictures and bladder outflow obstruction secondary to BPH.
The fourth generation
To avoid stent migration-related problems, scientists designed triangular prostatic Memokath stents. At first, these stents were cylindrical. The triangular shape conforms well to the prostatic urethral lumen shape, and no migrations occurred nine months after the procedure. More studies are necessary to evaluate the long-term potential of Memokath stents. Most research on this subject revolved around a relatively short follow-up period.
When talking about temporary stents, it’s also useful to mention other materials besides metal. Other materials include:
Plastic stents
The main representative is the Spanner stent, very similar to 4-6cm of a Foley catheter. The stent portion resides in the prostatic urethra, but the distal anchor resides in the bulbar urethra. Early experience with this device was encouraging. Later experience revealed that a significant percentage of patients had unsatisfactory outcomes such as irritation symptoms and urinary retention.
Biodegradable stents
Self-expandable stents include polylactic acid, polyglycolic acid, and copolymers of lactide and glycolide. The average degradation time ranges from two to 12 months. These stents degrade to CO2 and water without the need for removal. Biodegradable stents are usually coupled with 5-α-reductase inhibitors. Their main intention is to keep the obstructed prostatic lumen open until medication decreases the gland’s volume.
Just like permanent stents, temporary devices have certain benefits and shortcomings.
Let’s see what they are.
Advantages of the temporary prostatic stent
- Quick procedure (15 minutes), placed similarly to Foley catheter placement.
- Easy to remove, similar to the removal of a Foley catheter
- Patient retains volitional voiding
- More convenient option, according to patients, than Foley catheter
- Various temporary stents are available, including biodegradable that don’t require removal
Disadvantages of temporary prostate stents
- May cause mild discomfort.
- Patients may experience urinary retention or slight urinary incontinence if the stent is misplaced or the size is wrong.
- It doesn’t provide voiding function if the external sphincter and bladder don’t work properly, i.e., may not alleviate voiding symptoms.
- May lead to urinary frequency (which tends to go away within 78 hours)
- Risk of misplacement
Side effects
Let’s be honest; every procedure comes with a risk of certain side effects. The placement of the urethral stent isn’t the exception.
What can happen then?
Adverse reactions may vary from one person to another. That said, you may feel discomfort for the first few days after the procedure. Some men may experience a burning sensation as they pass urine.
These symptoms go away on their own after a few days. Consult your doctor if they are persistent.
As far as the device is concerned, you may have the need to urinate often and right away. Men with a prostate stent may also notice their urine is dribbling. Discomfort and light bleeding are also side effects of having a prostate stent.
Before the procedure, your urologist will explain everything. You’ll know how ureteral stent works, what to expect after surgery, and how to deal with potential side effects.
Conclusion
Prostate stents could be a beneficial treatment approach for men with BPH. The minimally-invasive procedure may involve permanent or temporary stent. They are made of metal, plastic, and biodegradable materials. Some patients may experience discomfort and problems affecting the lower urinary tract.
Not every patient with BPH is eligible for a prostatic stent. The successful outcome depends on the careful selection of the patients. Generally speaking, men eligible for this procedure are patients with severe symptoms but unable to undergo more invasive treatment types.
Biodegradable stents usually come in combination with medications. The choice of a stent depends on the severity of the symptoms you experience. The urologist will recommend the best option for your condition. The experience of the urologist also plays a role in the effectiveness of the treatment.
This article is for informational purposes only and does not serve as medical advice. The details provided here are not a replacement for, and should never be depended upon as, professional medical advice. Always consult your physician regarding the potential risks and benefits of any treatment.
Our Medical Review Process
At Ben’s Natural Health, we are committed to maintaining the highest standards of accuracy, transparency, and scientific integrity. Every piece of content is carefully developed by medical professionals and undergoes a thorough review every 12 to 24 months. This ensures that our information remains current, reliable, and rooted in credible, evidence-based research. We reference only peer-reviewed studies from reputable medical journals, providing full citations and direct links to enhance trust and confidence. Learn more about our medical review process and research standards.
Our Editorial Guidelines
For over 25 years, Ben’s Natural Health has been a trusted source of scientifically backed, reliable health information. Our editorial guidelines uphold the highest quality and integrity for every article we publish. Each piece is written by qualified experts and undergoes independent quality checks. We prioritize transparency by clearly displaying contributor credentials and biographies at the beginning of every article. Read more about our editorial standards.
Medical Disclaimer
The content on this blog is for informational purposes only and should not be considered a substitute for professional medical advice, diagnosis, or treatment. While our articles are authored and reviewed by licensed medical professionals, they may not address your specific health concerns. Always consult a qualified healthcare provider before making any medical decisions.
Article Sources
- Deters LA. (, 2019). How common is benign prostatic hyperplasia (BPH)? Medscape https://www.medscape.com/answers/437359-90389/how-common-is-benign-prostatic-hyperplasia-bph#:~:text=BPH%20is%20a%20common%20problem,have%20symptoms%20related%20to%20BPH.
- Samadi D. (2017). Treatment options for BPH: what is a prostatic stent? Prostate Cancer 911 https://prostatecancer911.com/treatment-options-for-bph-what-is-a-prostatic-stent/#:~:text=Prostatic%20stents%20are%20not%20considered,a%20high%20rate%20of%20complications.
- Lam, J. S., Volpe, M. A., & Kaplan, S. A. (2001). Use of prostatic stents for the treatment of benign prostatic hyperplasia in high-risk patients. Current urology reports, 2(4), 277–284. https://doi.org/10.1007/s11934-001-0064-2
- Corujo, M., & Badlani, G. H. (1997). Epithelialization of permanent stents. Journal of endourology, 11(6), 477–480. https://doi.org/10.1089/end.1997.11.477
- Vanderbrink, B. A., Rastinehad, A. R., & Badlani, G. H. (2007). Prostatic stents for the treatment of benign prostatic hyperplasia. Current opinion in urology, 17(1), 1–6. https://doi.org/10.1097/MOU.0b013e3280117747
- De Vocht, T. F., van Venrooij, G. E., & Boon, T. A. (2003). Self-expanding stent insertion for urethral strictures: a 10-year follow-up. BJU international, 91(7), 627–630. https://doi.org/10.1046/j.1464-410x.2003.04200.x
- Masood, S., Djaladat, H., Kouriefs, C., Keen, M., & Palmer, J. H. (2004). The 12-year outcome analysis of an endourethral wall stent for treating benign prostatic hyperplasia. BJU international, 94(9), 1271–1274. https://doi.org/10.1111/j.1464-410X.2004.05155.x
- Tomschi, W., & Lüftenegger, W. (1990). Die urologische Spirale. Eine echte Alternative zum Verweilkatheter? Erfahrungsbericht an 23 Patienten [The urological spiral. A real alternative to the indwelling catheter? Experience in 23 patients]. Wiener klinische Wochenschrift, 102(21), 650–653.
- Yachia, D., & Aridogan, I. A. (1996). Comparison between first-generation (fixed-caliber) and second-generation (self-expanding, large caliber) temporary prostatic stents. Urologia internationalis, 57(3), 165–169. https://doi.org/10.1159/000282903
- Sethi, K., Bozin, M., Jabane, T., McMullin, R., Cook, D., Forsyth, R., Dodds, L., & Putra, L. J. (2017). Thermo-expandable prostatic stents for bladder outlet obstruction in the frail and elderly population: An underutilized procedure?. Investigative and clinical urology, 58(6), 447–452. https://doi.org/10.4111/icu.2017.58.6.447
- van Dijk, M. M., Mochtar, C. A., Wijkstra, H., Laguna, M. P., & de la Rosette, J. J. (2005). Hourglass-shaped nitinol prostatic stent in the treatment of patients with lower urinary tract symptoms due to bladder outlet obstruction. Urology, 66(4), 845–849. https://doi.org/10.1016/j.urology.2005.04.030
- Marković, B. B., Marković, Z., Yachia, D., & Hadzi, D. J. (2007). Acta chirurgica Iugoslavica, 54(3), 71–76. https://doi.org/10.2298/aci0703071m
- Grimsley, S. J., Khan, M. H., Lennox, E., & Paterson, P. H. (2007). Experience with the spanner prostatic stent in patients unfit for surgery: an observational study. Journal of endourology, 21(9), 1093–1096. https://doi.org/10.1089/end.2006.0254
Article Update History
Updated on 30 May, 2026 (Current Version)
Created on 30 September, 2020
Explore More

Prostatitis Statistics: Key Facts and Insights in 2026
Prostatitis, an inflammatory condition of the prostate gland, remains a key health concern worldwide. In 2026, a deeper understanding of its prevalence, types, diagnosis, ...