- Q: Who should get PSA tested?
- Q: What causes PSA elevation in the blood?
- Q: How often should a PSA test be done?
- Q: What are the limitations of PSA screening?
- Q: What is the relationship between prostate cancer and the PSA test?
- Q: What are the potential benefits and harms of PSA screening?
- Q: What is the difference between Free and Total PSA?
- Q: What about PSA density, velocity, and age-related PSA considerations?
- Q: What do PSA test results mean?
- Q: What are other tests available for prostate cancer screening?
- Top FAQs on PSA Testing and Normal PSA Levels
- Conclusion
- Our Medical Review Process
- Our Editorial Guidelines
- Medical Disclaimer
- Source
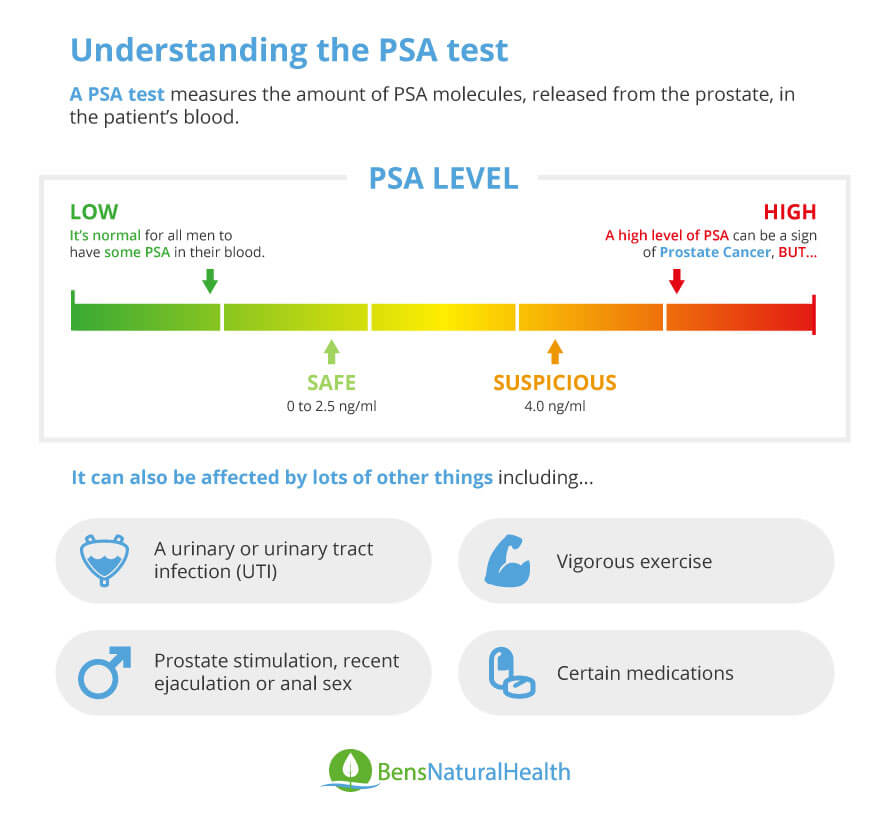
If you’re a man over 50, you’ve probably had your doctor recommend a PSA test during your annual exam, or you may have already undergone one. PSA, or prostate-specific antigen, is a protein made by the prostate gland, and the PSA test measures the level of this protein in your blood.
Approved by the FDA in 1986, the PSA test quickly became a standard part of routine blood work. However, with widespread screening, the number of men diagnosed with prostate cancer also rose significantly, leading to both earlier detections and concerns about overdiagnosis.
But what is a PSA test exactly? To help us better understand PSA testing, its benefits, limitations, and the decisions surrounding it, we spoke with Dr. Menna Salman, a renowned urologist specializing in prostate health. Throughout this article, Dr. Salman offers insights supported by medical research and clinical experience to help men make informed decisions about their prostate health.
Get Your FREE PSA Lowering Diet Plan!
- Naturally lower PSA levels
- Reduce nighttime trips to the bathroom
- Enjoy better bladder control and urine flow
Q: Who should get PSA tested?
Dr. Salman answers: A cancerous growth inside the prostate can certainly cause PSA levels to rise significantly. However, many other factors can also cause an increase. Typically, we recommend PSA screening for all men over 50.
That said, guidelines vary. The U.S. Preventive Services Task Force (USPSTF) advises against routine PSA screening in healthy men over 70 with no symptoms. Some experts also suggest avoiding screening in symptomless men at low risk for prostate cancer.
Q: What causes PSA elevation in the blood?
Dr. Salman answers: A number of different things can cause an elevated PSA reading, not just cancer. Some common causes include:
- Prostatitis (prostate inflammation)
- A urinary infection
- Recent or intense sexual activity
- Bicycle or horseback riding
- Benign prostatic hyperplasia (BPH), or an enlarged prostate
- Aging
- A recent digital rectal exam (DRE)
It’s quite common for a man to have a temporary PSA elevation that drops back to normal within a few weeks. If a PSA reading comes back elevated during an annual exam, I usually recommend repeating the test in about 60 to 90 days. If the second test confirms the elevation or shows an even higher result, that’s when we consider further evaluation.
Keeping a personal record of PSA levels over the years is smart. It helps both the patient and the doctor spot trends instead of reacting to a single unusual result. For example, older men with a history of BPH often show a slow PSA rise over time, which is less concerning than a sudden spike.
While PSA alone isn’t specific for cancer, when combined with a long-term record, it provides valuable context that can sometimes prevent unnecessary biopsies. However, when suspicion remains, a biopsy is the only reliable way to confirm a prostate cancer diagnosis.
Q: How often should a PSA test be done?
Dr. Salman answers: There’s no universal schedule for PSA testing. Most doctors recommend annual screenings starting at age 50 for men at average risk.
An elevated PSA reading often leads to a biopsy, which carries its own risks, so it’s important to individualize decisions. Recently, the USPSTF updated their recommendation to exclude men over 70 from routine screening.
Ultimately, deciding when and how often to screen should be a shared decision between a man and his doctor, based on health status, age, and previous PSA history.
Q: What are the limitations of PSA screening?
Dr. Salman answers: PSA screening is often automatically included in blood work during annual exams, especially for men over 50. While it’s a simple blood test with no direct risks, the consequences of an abnormal result can lead to unnecessary anxiety and procedures.
The baseline PSA value established early on can be very useful for comparison in future tests. Some men’s PSA levels remain steady as they age, while others see a natural rise.
The USPSTF advises that for men aged 55 to 69, PSA screening should involve a detailed discussion about the pros and cons. An elevated PSA could result in further tests and even biopsies, which carry their own risks like infection, bleeding, and emotional stress.
It’s important to remember: while prostate biopsies can find cancer early, they can also miss it. And treating non-aggressive cancers aggressively can sometimes do more harm than good.

Q: What is the relationship between prostate cancer and the PSA test?
Dr. Salman answers: Prostate cancer is one of the most commonly diagnosed cancers in older men. A man has about a 1-in-6 chance of being diagnosed during his lifetime. Thankfully, it’s often very slow-growing.
Only about 10% of cases are aggressive enough to be life-threatening. Many older men diagnosed with prostate cancer will have other, more pressing health issues.
Elevated PSA doesn’t necessarily mean cancer. BPH, prostatitis, or a UTI can also elevate PSA levels. Conversely, normal PSA levels don’t guarantee you’re cancer-free.
Unfortunately, a single elevated PSA often leads to a biopsy, and finding any cancer can lead to aggressive treatment, even when “watchful waiting” might be the better approach. That’s why I always stress that a diagnosis should be used as information for thoughtful decision-making, not as an automatic trigger for surgery or radiation.
Q: What are the potential benefits and harms of PSA screening?
Dr. Salman answers: The primary goal of PSA screening is to detect aggressive prostate cancers early enough for effective treatment.
However, false positives are very common, especially in older men, leading to unnecessary biopsies and sometimes overtreatment.
Biopsies themselves can cause infections, blood in the semen or urine, erectile dysfunction, and pain. Infection is especially concerning, occurring in over 7% of biopsy patients and occasionally resulting in hospitalization or even life-threatening sepsis.
So, while early detection can save lives, it also carries risks that must be carefully weighed.

Q: What is the difference between Free and Total PSA?
Dr. Salman answers: In the bloodstream, PSA exists in two forms: “total PSA,” which is bound to other proteins, and “free PSA,” which circulates freely.
In a healthy prostate, over 25% of the PSA is free. In a cancerous prostate, the percentage of free PSA drops, often below 10–12%.
Unfortunately, many doctors only order the total PSA test, but ordering both free and total PSA provides much better information. Since they can be measured from the same blood sample, I see no reason not to request both.
It’s critical for men to understand that an elevated PSA doesn’t equal a cancer diagnosis, and that additional factors like free PSA percentages should be part of the decision-making process.

Q: What about PSA density, velocity, and age-related PSA considerations?
Dr. Salman answers: Benign Prostatic Hyperplasia (BPH), or prostate enlargement, is very common in older men and usually harmless unless it causes urinary issues.
Generally, a larger prostate produces more PSA. PSA density adjusts the PSA level to the size of the prostate, giving a more accurate picture.
PSA also naturally tends to rise with age, though there are no universally accepted age-specific normal ranges.
Another key concept is PSA velocity, how quickly the PSA level rises year after year. If it rises slowly (less than 0.75 ng/mL annually), it’s usually less worrisome. But a rapid rise could signal trouble and warrants immediate follow-up.
Waiting 60 days and retesting after an initial high PSA is often a wise move, especially if temporary causes like infection are suspected.

Q: What do PSA test results mean?
Dr. Salman answers: If a follow-up test shows a significant drop in PSA, the initial rise was probably due to external factors like recent cycling, sexual activity, or infection.
If PSA rises by more than a point or continues climbing, it raises concern about a potential tumor, and further investigation is necessary.

Q: What are other tests available for prostate cancer screening?
Dr. Salman answers: One newer test is the Prostate Cancer Antigen 3 (PCA3) test. This test looks for a genetic marker produced only by prostate cells, and cancerous cells produce much higher amounts.
The PCA3 test involves a digital rectal exam followed by a urine sample collection. The PCA3 score gives an indication of the likelihood of finding prostate cancer on a biopsy.
While helpful, the PCA3 is not a substitute for PSA testing or biopsy, it’s just another tool to help guide decision-making, especially for men under “watchful waiting.”
Top FAQs on PSA Testing and Normal PSA Levels
Q: Can certain medications lower PSA levels artificially and mask prostate issues?
Dr. Salman answers: Some drugs can lower PSA levels and mask the prostate issues, such as finasteride (Proscar) and dutasteride (Avodart). These drugs are used in cases of BPH and can lower PSA levels by about 50% after use for about 6-12 months. This lowering in the PSA level occurs as these drugs can shrink the prostate and lower PSA production; it is not always related to any decline in cancer risk. As research shows, other medications such as NSAIDs, statins, and thiazide diuretics may also reduce PSA levels.
So, if the drug usage isn’t asked about before testing for PSA, this might result in false results and interpretation.
Q: Does alcohol consumption affect PSA levels before a test?
Dr. Salman answers: While excessive drinking could harm prostate health, moderate alcohol use has no impact on PSA levels.
Studies have shown that there is no direct increase in PSA levels after drinking alcohol before a test. However, it is preferred to avoid alcohol drinking 24 hours before PSA level testing to avoid any possible effect on the results because alcohol can affect the hydration and liver metabolism.
On the other hand, persistent excessive drinking could cause hormone imbalances, liver damage, and general inflammation that might affect prostate health. Long-term excessive alcohol use has also been linked to an increased risk of aggressive prostate cancer.
Q: What are the risks of delaying a biopsy after a high PSA?
Dr. Salman answers: Delaying a biopsy after a high PSA test result might raise the chance of missing an early-stage prostate cancer diagnosis. Prostate cancer is usually a slowly growing tumor, but it may become more aggressive over time. So, delaying the diagnosis may lead to the spread of prostate cancer. The disease will be more advanced and the treatment, such as surgery or radiation, may become less effective and have more side effects.
However, note that not every high PSA result means that there is prostate cancer; some may occur due to BPH or prostatitis. So, the need for a biopsy is based on a careful assessment of other elements, such as your age, general health, and any other symptoms you might be having.
Q: How accurate is MRI for detecting prostate cancer compared to PSA screening alone?
Dr. Salman answers: Studies showed that MRI, especially multiparametric MRI (mpMRI), can be more accurate in detecting prostate cancer than doing a PSA screening test alone. While PSA is considered the best first-line test (screening test), it may lead to unnecessary prostate biopsies. MRI, on the other hand, offers a detailed view of the prostate and can identify any tumors that PSA might miss. Studies found that MRI can detect about 63% of prostate cancers.
Q: Are there new imaging technologies that can reduce reliance on biopsies after elevated PSA?
Dr. Salman answers: While a prostate biopsy is still the main way to confirm if someone has prostate cancer, newer imaging tests—especially multiparametric MRI (mpMRI)—are helping doctors decide who really needs one. These scans give a clearer picture of the prostate and can often tell if something looks suspicious. If the MRI doesn’t show anything concerning, some men can safely skip the biopsy altogether. New tools like PSMA PET scans and high-resolution ultrasound are also being developed and might reduce the need for unnecessary biopsies even more in the future.
Q: What role does diet and nutrition play in PSA levels?
Dr. Salman answers: While diet isn’t a replacement for screening or treatment, it’s a valuable piece of the puzzle to protect your prostate health.
Diets rich in fruits, vegetables, whole grains, and healthy fats, like those from fish, nuts, and olive oil, are linked to lower inflammation and may help stabilize PSA levels.
Specific foods like tomatoes (which contain lycopene), green tea, and soy products have shown promise in supporting prostate health due to their antioxidant and anti-inflammatory effects.
On the other side, regular eating of red or processed meats, high-fat dairy, and sugary foods may raise PSA and possibly increase your risk of prostate issues.
Conclusion
The PSA test is a valuable early warning tool, but it should be treated as a piece of the puzzle, not a definitive answer. It’s important not to rush into aggressive treatment based solely on PSA levels.
Research shows that many prostate surgeries may be unnecessary, and their side effects, including urinary incontinence and sexual dysfunction, can seriously impact quality of life.
In short, PSA testing should open a conversation, not close it. Proper interpretation and a cautious, informed approach are essential.
Our Medical Review Process
At Ben’s Natural Health, we prioritize accuracy, transparency, and scientific integrity in all of our content. Each article is developed by qualified medical professionals and undergoes a comprehensive review every 12 to 24 months to ensure it remains up to date and evidence-based. We reference only peer-reviewed studies from respected medical journals, with full citations and direct links included to support our commitment to credibility.[Learn more about our medical review process and research standards.
Our Editorial Guidelines
For over 25 years, Ben’s Natural Health has been a reliable source of science-backed natural health information. Our editorial guidelines ensure that every article meets the highest standards of accuracy and trustworthiness. Content is written by certified professionals—including doctors, dietitians, nutritionists, fitness experts, and surgeons—and independently reviewed for medical accuracy. To promote transparency, we include contributor bios and credentials at the top of each article. Read more about our editorial standards.
Medical Disclaimer
The information provided on this site is for general educational purposes only and is not intended as a substitute for professional medical advice, diagnosis, or treatment. While our content is created and reviewed by licensed healthcare professionals, it may not be tailored to your specific health needs. Always consult your doctor or a qualified healthcare provider before making any health-related decisions. Never disregard or delay seeking professional medical advice because of information found on this site. Use of this content is at your own risk.